

2017 Chitranjan S. Ranawat Award: Does Computer Navigation in Knee Arthroplasty Improve Functional Outcomes in Young Patients? A Randomized Study
- PMID: 29389753
- PMCID: PMC5919243
- DOI: 10.1007/s11999.0000000000000000
2017 Chitranjan S. Ranawat Award: Does Computer Navigation in Knee Arthroplasty Improve Functional Outcomes in Young Patients? A Randomized Study
Abstract
Background: Proponents of computer-assisted TKA suggest that better alignment of the TKAs will lead to improved long-term patient functional outcome and survivorship of the implants. However, there is little evidence about whether the improved position and alignment of the knee components obtained using computer navigation improve patient function and the longevity of the TKA.
Questions/purposes: The purpose of this study was to determine whether (1) clinical results; (2) radiographic and CT scan results; and (3) the survival rate of TKA components would be better in patients having computer-assisted TKA than results of patients having TKA without computer-assisted TKA. In addition, we determined whether (4) complication rates would be less in the patients with computer-assisted TKA than those in patients with conventional TKA.
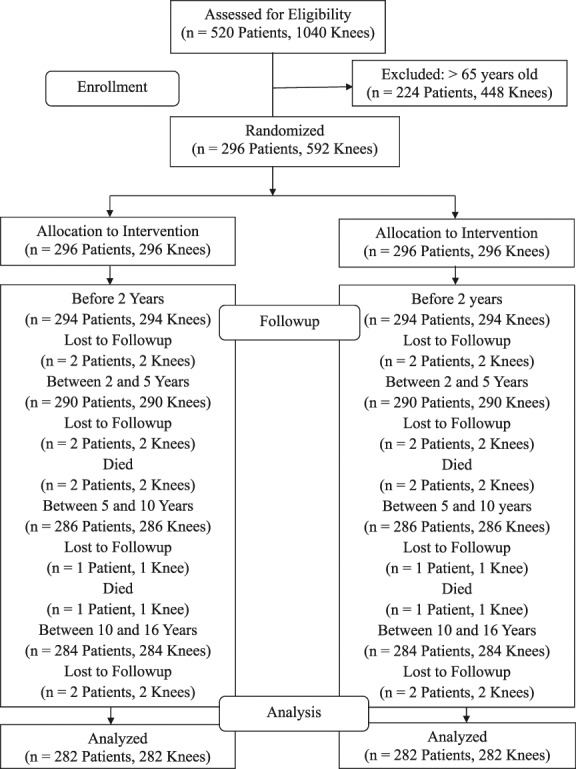
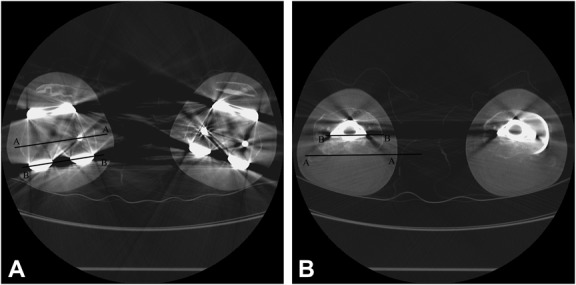
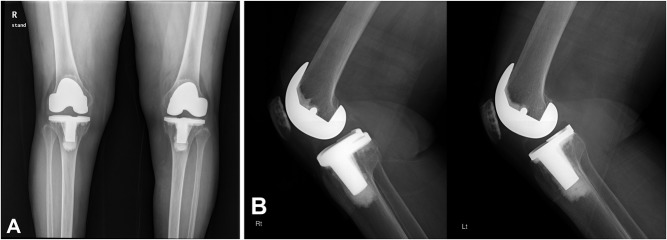
Methods: We performed a randomized trial between October 2000 and October 2002 in patients undergoing same-day bilateral TKA; in this trial, one knee was operated on using navigation, and the other knee was operated on without navigation. All 296 patients who underwent same-day bilateral TKA during that period were enrolled. Of those, 282 patients (95%) were accounted for at a mean of 15 years (range, 14-16 years). A total of 79% (223 of 282) were women and the mean age of the patients at the time of index arthroplasty was 59 ± 7 years (range, 48-64 years). Knee Society knee score, WOMAC score, and UCLA activity score were obtained preoperatively and at latest followup. Radiographic measurements were performed including femorotibial angle, position of femoral and tibial components, level of joint line, and posterior condylar offset. Aseptic loosening was defined as a complete radiolucent line > 1 mm in width around any component or migration of any component. Assessors and patients were blind to treatment assignment.
Results: The Knee Society knee (92 ± 8 versus 93 ± 7 points; 95% confidence interval [CI], 92-98; p = 0.461) and function scores (80 ± 11 versus 80 ± 11 points; 95% CI, 73-87; p = 1.000), WOMAC score (14 ± 7 versus 15 ± 8 points; 95% CI, 14-18; p = 0.991), range of knee motion (128° ± 9° versus 127° ± 10°; 95% CI, 100-140; p = 0.780), and UCLA patient activity score (6 versus 6 points; 95% CI, 4-8; p = 1.000) were not different between the two groups at 15 years followup. There were no differences in any radiographic parameters of alignment (on radiography or CT scan) between the two groups. The frequency of aseptic loosening was not different between the two groups (p = 0.918). Kaplan-Meier survivorship of the TKA components was 99% in both groups (95% CI, 93-100) at 15 years as the endpoint of revision or aseptic loosening (p = 0.982). Anterior femoral notching was observed in 11 knees (4%) in the computer-assisted TKA group and none in the conventional TKA group (p = 0.046).
Conclusions: In this randomized trial, with data presented at a minimum of 14 years of followup, we found no benefit to computer navigation in TKA in terms of pain, function, or survivorship. Unless another study at long-term followup identifies an advantage to survivorship, pain, and function, we do not recommend the widespread use of computer navigation in TKA because of its risks (in this series, we observed femoral notching; others have observed pin site fractures) and attendant costs.
Level of evidence: Level I, therapeutic study.
Conflict of interest statement
Each author certifies that neither he, nor any member of his immediate family, have funding or commercial associations (consultancies, stock ownership, equity interest, patent/licensing arrangements, etc) that might pose a conflict of interest in connection with the submitted article.
All ICMJE Conflict of Interest Forms for authors and
Figures
Comment in
-
Letter to the Editor: 2017 Chitranjan S. Ranawat Award: Does Computer Navigation in Knee Arthroplasty Improve Functional Outcomes in Young Patients? A Randomized Study.Clin Orthop Relat Res. 2018 Jun;476(6):1362-1363. doi: 10.1007/s11999.0000000000000305. Clin Orthop Relat Res. 2018. PMID: 29629936 Free PMC article. No abstract available.
-
Reply to the Letter to the Editor: 2017 Chitranjan S. Ranawat Award: Does Computer Navigation in Knee Arthroplasty Improve Functional Outcomes in Young Patients? A Randomized Study.Clin Orthop Relat Res. 2018 Jun;476(6):1364. doi: 10.1007/s11999.0000000000000306. Clin Orthop Relat Res. 2018. PMID: 29629937 Free PMC article. No abstract available.
-
In Younger Patients with End-Stage Knee Osteoarthritis, Computer-Assisted Versus Conventional Total Knee Arthroplasty Did Not Improve Function at 15 Years.J Bone Joint Surg Am. 2018 Nov 21;100(22):1982. doi: 10.2106/JBJS.18.00917. J Bone Joint Surg Am. 2018. PMID: 30480602 No abstract available.
References
-
- Ahlbäck S. Osteoarthrosis of the knee: a radiographic investigation. Acta Radiol Diagn (Stockh). 1968;277(Suppl):7–72. - PubMed
-
- Arima J, Whiteside LA, McCarthy DS, Shite SE. Femoral rotational alignment, based on the anteroposterior axis, in total knee arthroplasty in a valgus knee. A technical note. J Bone Joint Surg Am. 1995;77:1331–1334. - PubMed
-
- Bäthis H, Perlick L, Tingart M, Luring C, Zurakowski D, Grifka J. Alignment in total knee arthroplasty. A comparison of computer-assisted surgery with the conventional technique. J Bone Joint Surg Br. 2004;86:682–687. - PubMed
-
- Baumbach JA, Willburger R, Haaker R, Dittrich M, Kohler S. 10-year survival of navigated versus conventional TKAs: a retrospective study. Orthopedics. 2016;39:S72–S76. - PubMed
-
- Bauwens K, Matthes G, Wich M, Gebhard F, Hanson B, Ekkernkamp A, Stengel D. Navigated total knee replacement. A meta-analysis. J Bone Joint Surg Am. 2007;89:261–269. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
