

Comparison of safety and effectiveness between laparoscopic mini-gastric bypass and laparoscopic sleeve gastrectomy: A meta-analysis and systematic review
- PMID: 29390281
- PMCID: PMC5815693
- DOI: 10.1097/MD.0000000000008924
Comparison of safety and effectiveness between laparoscopic mini-gastric bypass and laparoscopic sleeve gastrectomy: A meta-analysis and systematic review
Abstract
Background: The laparoscopic mini-gastric bypass is a newly emerged surgical procedure in recent years. Owe to safe and simple process and effective outcomes, laparoscopic mini-gastric bypass has quickly become one of the most popular procedures in some countries. The safety and effectiveness of laparoscopic mini-gastric bypass versus laparoscopic sleeve gastrectomy remain unclear.
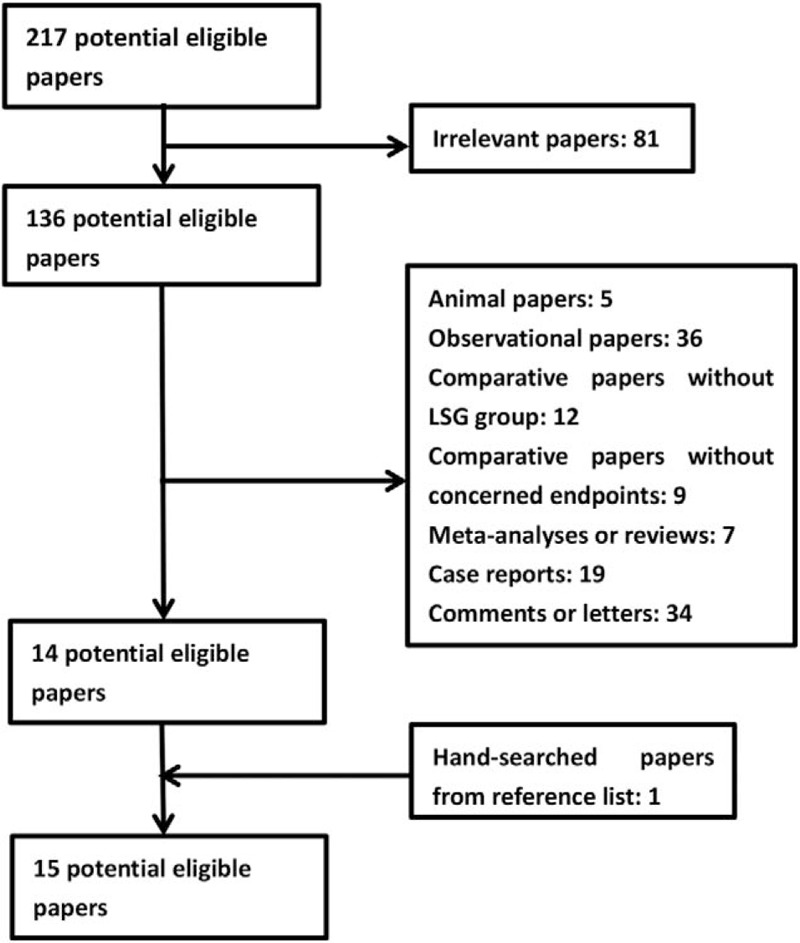
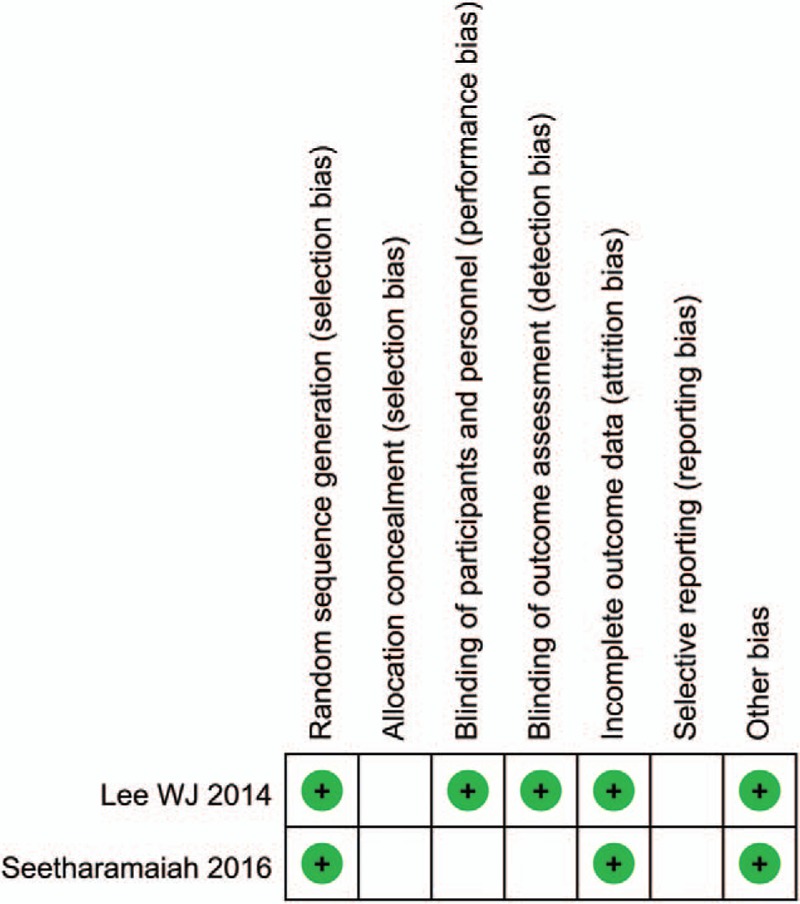
Methods: A systematic literature search was performed in PubMed, Embase, Cochrane library from inception to May 20, 2017. The methodological quality of Randomized Controlled Trials and non-Randomized Controlled Trials were, respectively, assessed by Cochrane Collaboration's tool for assessing risk of bias and Newcastle-Ottawa scale. The meta-analysis was performed by RevMan 5.3 software.
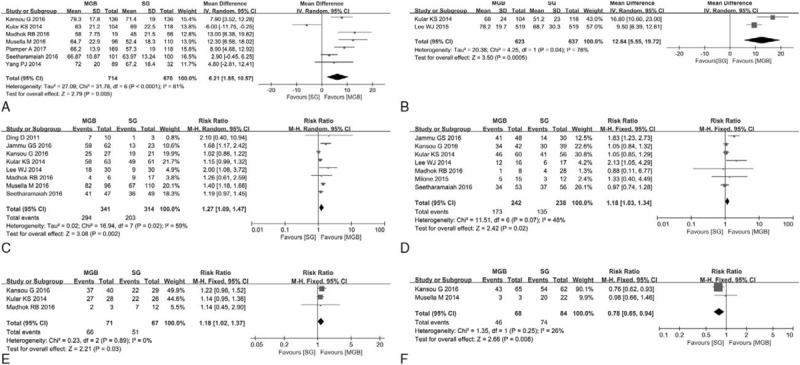
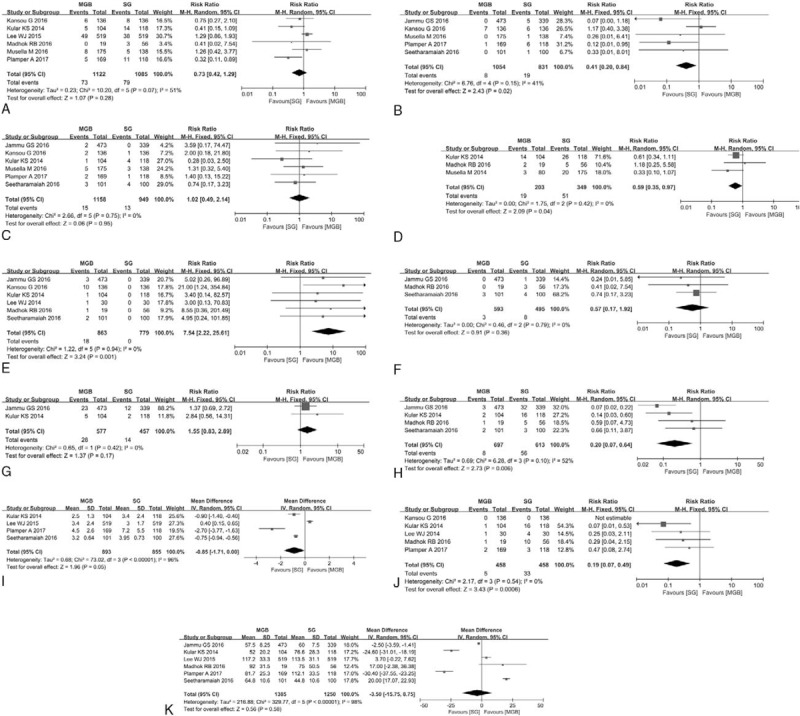
Results: Patients receiving mini-gastric bypass had a lot of advantageous indexes than patients receiving sleeve gastrectomy, such as higher 1-year EWL% (excess weight loss), higher 5-year EWL%, higher T2DM remission rate, higher hypertension remission rate, higher obstructive sleep apnea (OSA) remission rate, lower osteoarthritis remission rate, lower leakage rate, lower overall late complications rate, higher ulcer rate, lower gastroesophageal reflux disease (GERD) rate, shorter hospital stay and lower revision rate. No significant statistical difference was observed on overall early complications rate, bleed rate, vomiting rate, anemia rate, and operation time between mini-gastric bypass and sleeve gastrectomy.
Conclusion: Mini-gastric bypass is a simpler, safer, and more effective bariatric procedure than laparoscopic sleeve gastrectomy. Due to the biased data, small sample size and short follow-up time, our results may be unreliable. Large sample and multicenter RCT is needed to compare the effectiveness and safety between mini-gastric bypass and sleeve gastrectomy. Future study should also focus on bile reflux, remnant gastric cancer, and long term effectiveness of mini-gastric bypass.
Copyright © 2017 The Authors. Published by Wolters Kluwer Health, Inc. All rights reserved.
Conflict of interest statement
The authors have no funding and no conflicts of interest to disclose.
Figures
References
-
- Ogden CL, Carroll MD, Kit BK, et al. Prevalence of obesity among adults: United States, 2011–2012. NCHS Data Brief 2013;1–8. - PubMed
-
- Fontaine KR, Redden DT, Wang C, et al. Years of life lost due to obesity. JAMA 2003;289:187–93. - PubMed
-
- Abegunde DO, Mathers CD, Adam T, et al. The burden and costs of chronic diseases in low-income and middle-income countries. Lancet 2007;370:1929–38. - PubMed
-
- Buchwald H, Avidor Y, Braunwald E, et al. Bariatric surgery: a systematic review and meta-analysis. JAMA 2004;292:1724–37. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
