

Delayed onset Mycobacterium intracellulare keratitis after laser in situ keratomileusis: A case report and literature review
- PMID: 29390522
- PMCID: PMC5758224
- DOI: 10.1097/MD.0000000000009356
Delayed onset Mycobacterium intracellulare keratitis after laser in situ keratomileusis: A case report and literature review
Abstract
Rationale: Infectious keratitis is a relatively uncommon but potentially sight-threatening complication of laser in situ keratomileusis (LASIK). Mycobacterial keratitis is usually regarded as late onset keratitis among post-LASIK keratitis. There has been no documented case of Mycobacterium intracellulare post-LASIK keratitis of a long-latent period.
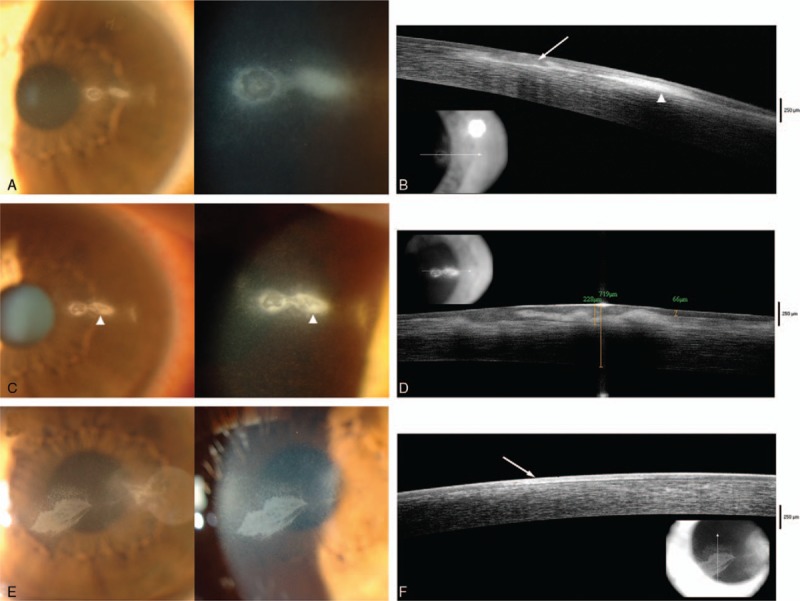
Patient concerns: A 36-year-old man was referred to our out-patient clinic, for persistent corneal epithelial defect with intrastromal infiltration. He had undergone uneventful bilateral LASIK procedure 4 years before. He complained decreased vision, accompanied by ocular pain, photophobia, and redness in his left eye for 7 months.
Diagnosis: Lamellar keratectomy was taken using femtosecond laser. Bacterial culture with sequenced bacterial 16s ribosomal DNA confirmed the organism to be M intracellulare.
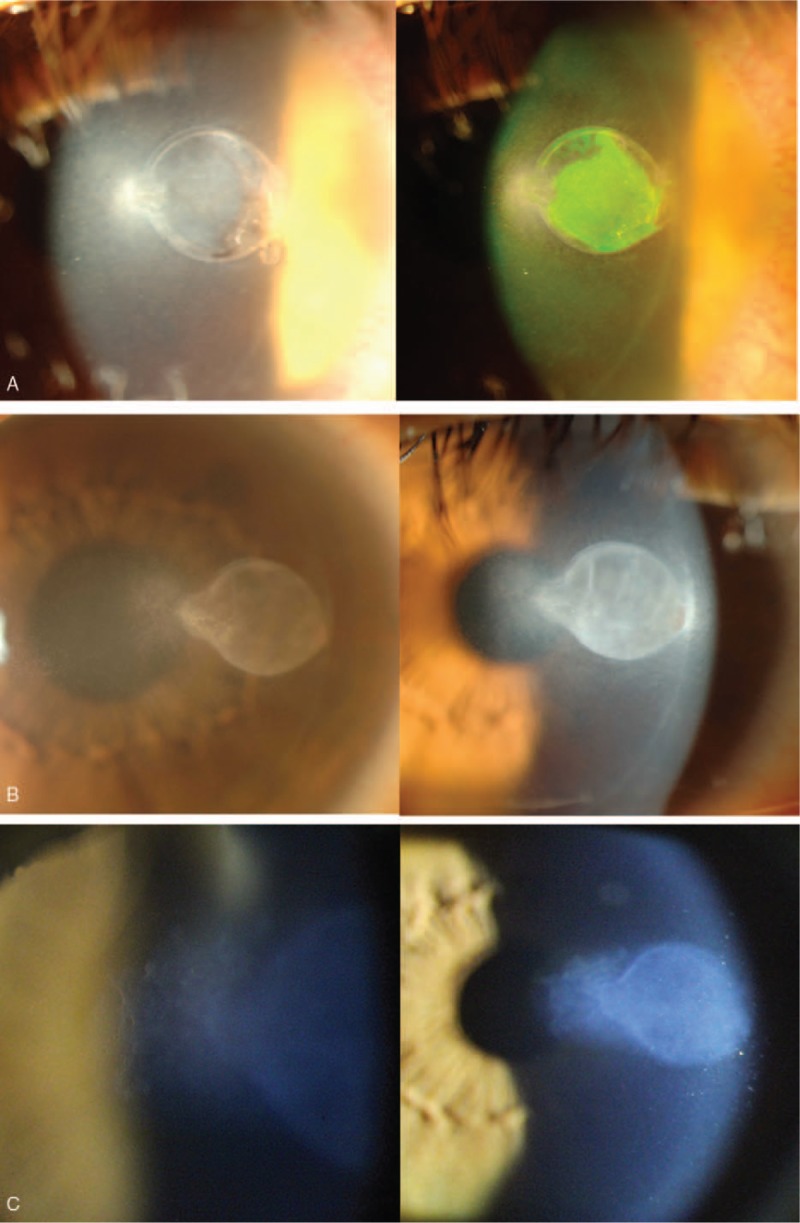
Interventions: After 3 months of administration of topical clarithromycin, amikacin, and moxifloxacin, the corneal epithelial defect was resolved and the infiltration was much improved. However, newly developed diffuse haziness with surrounding granular infiltration in the central cornea was noted. Drug toxicity was suspected and topical moxifloxacin was discontinued, resulting in resolution of the diffuse haze with infiltration.
Outcome: The patient was followed up regularly without medication thereafter and recurrence was not found for 7 years.
Lessons: This case presents the first case of M intracellulare keratitis after LASIK. LASIK surgeons should aware that post-LASIK keratitis can develop long after the operation and careful suspicion of infectious disease with meticulous diagnostic test is needed.
Copyright © 2017 The Authors. Published by Wolters Kluwer Health, Inc. All rights reserved.
Conflict of interest statement
EKK is the medical advisory board member of the Avellino LAB USA. Other authors have no conflicts of interest to declare.
The authors have no conflicts of interest to disclose.
Figures
References
-
- John T, Velotta E. Nontuberculous (atypical) mycobacterial keratitis after LASIK: current status and clinical implications. Cornea 2005;24:245–55. - PubMed
-
- Fulcher SF, Fader RC, Rosa RH, Jr, et al. Delayed-onset mycobacterial keratitis after LASIK. Cornea 2002;21:546–54. - PubMed
-
- Chung MS, Goldstein MH, Driebe WT, Jr, et al. Mycobacterium chelonae keratitis after laser in situ keratomileusis successfully treated with medical therapy and flap removal. Am J Ophthalmol 2000;129:382–4. - PubMed
-
- Daines BS, Vroman DT, Sandoval HP, et al. Rapid diagnosis and treatment of mycobacterial keratitis after laser in situ keratomileusis. J Cataract Refract Surg 2003;29:1014–8. - PubMed
-
- Chung SH, Roh MI, Park MS, et al. Mycobacterium abscessus keratitis after LASIK with IntraLase femtosecond laser. Ophthalmologica 2006;220:277–80. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
