

Financial Incentives for Chronic Disease Management: Results and Limitations of 2 Randomized Clinical Trials With New York Medicaid Patients
- PMID: 29390862
- PMCID: PMC7256969
- DOI: 10.1177/0890117117753986
Financial Incentives for Chronic Disease Management: Results and Limitations of 2 Randomized Clinical Trials With New York Medicaid Patients
Abstract
Purpose: To identify whether financial incentives promote improved disease management in Medicaid recipients diagnosed with hypertension or diabetes, respectively.
Design: Four-group, multicenter, randomized clinical trials.
Setting and participants: Between 2013 and 2016, New York State Medicaid managed care members diagnosed with hypertension (N = 920) or with diabetes (N = 959).
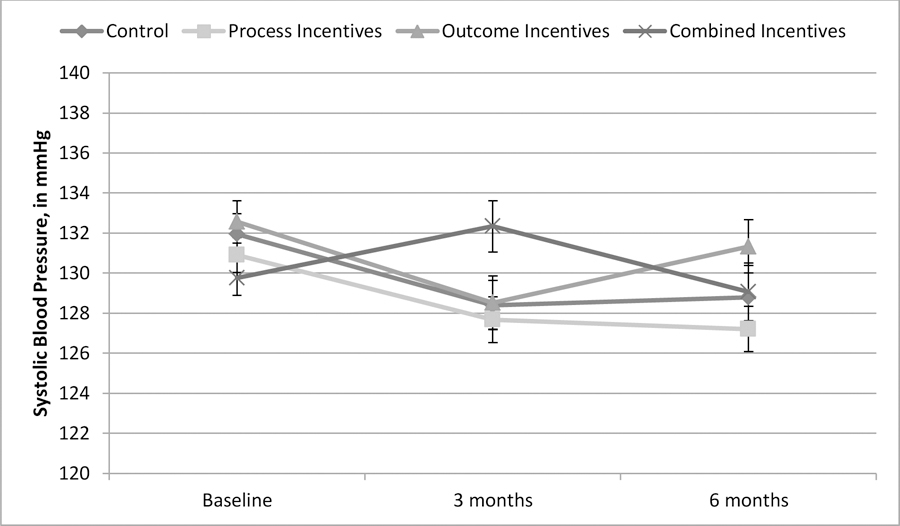
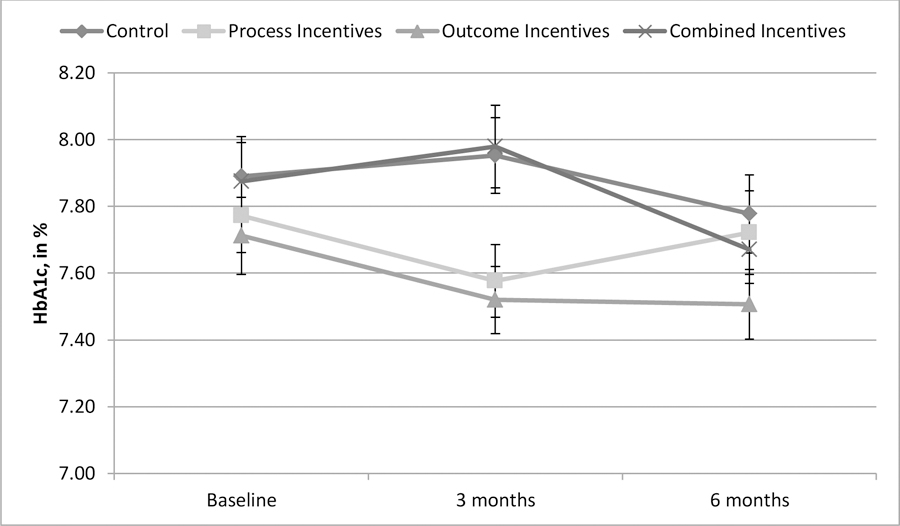
Intervention: Participants in each 6-month trial were randomly assigned to 1 of 4 arms: (1) process incentives-earned by attending primary care visits and/or receiving prescription medication refills, (2) outcome incentives-earned by reducing systolic blood pressure (hypertension) or hemoglobin A1c (HbA1c; diabetes) levels, (3) combined process and outcome incentives, and (4) control (no incentives).
Measures: Systolic blood pressure (hypertension) and HbA1c (diabetes) levels, primary care visits, and medication prescription refills. Analysis and Results: At 6 months, there were no statistically significant differences between intervention arms and the control arm in the change in systolic blood pressure, P = .531. Similarly, there were no significant differences in blood glucose control (HbA1c) between the intervention arms and control after 6 months, P = .939. The majority of participants had acceptable systolic blood pressure (<140 mm Hg) or blood glucose (<8.0%) levels at baseline and throughout the study.
Conclusion: Financial incentives-regardless of whether they were delivered based on disease-relevant outcomes, process activities, or a combination of the two-have a negligible impact on health outcomes for Medicaid recipients diagnosed with either hypertension or diabetes in 2 studies in which, among other design and operational limitations, the majority of recipients had relatively well-controlled diseases at the time of enrollment.
Keywords: diabetes; financial incentives; hypertension; incentives; interventions; medicaid; motivation; outcomes; population health; process; strategies.
Figures
References
-
- Gerteis J, Izrael D, Deitz D, LeRoy L, Ricciardi R, Miller T, Basu J. Multiple Chronic Conditions Chartbook.[PDF - 10.62 MB] AHRQ Publications No, Q14–0038. Rockville, MD: Agency for Healthcare Research and Quality; 2014.
-
- Elzubier AG, Husain AA, Suleiman IA, Hamid ZA. Drug compliance among hypertensive patients in Kassala, eastern Sudan. East Mediter Health J 2000;6:100–105. - PubMed
-
- DiMatteo MR, Giordani PJ, Lepper HS, Croghan TW. Patient adherence and medical treatment outcomes: A meta-analysis. Med Care 2002;40(9):794–811. - PubMed
-
- Croke AS. The faces of Medicaid: The complexities of caring for people with chronic illnesses and disabilities. Hamilton, NJ: Center for Health Care Strategies, Inc. 2000.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
