

Adherence to home fortification with micronutrient powders in Kenyan pre-school children: self-reporting and sachet counts compared to an electronic monitoring device
- PMID: 29391008
- PMCID: PMC5796300
- DOI: 10.1186/s12889-018-5097-2
Adherence to home fortification with micronutrient powders in Kenyan pre-school children: self-reporting and sachet counts compared to an electronic monitoring device
Abstract
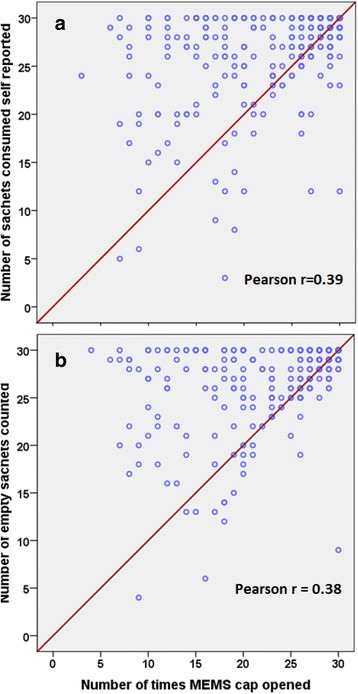
Background: The efficacy of home fortification with iron-containing micronutrient powders varies between trials, perhaps in part due to population differences in adherence. We aimed to assess to what extent adherence measured by sachet count or self-reporting forms is in agreement with adherence measured by electronic device. In addition, we explored how each method of adherence assessment (electronic device, sachet count, self-reporting forms) is associated with haemoglobin concentration measured at the end of intervention; and to what extent baseline factors were associated with adherence as measured by electronic device.
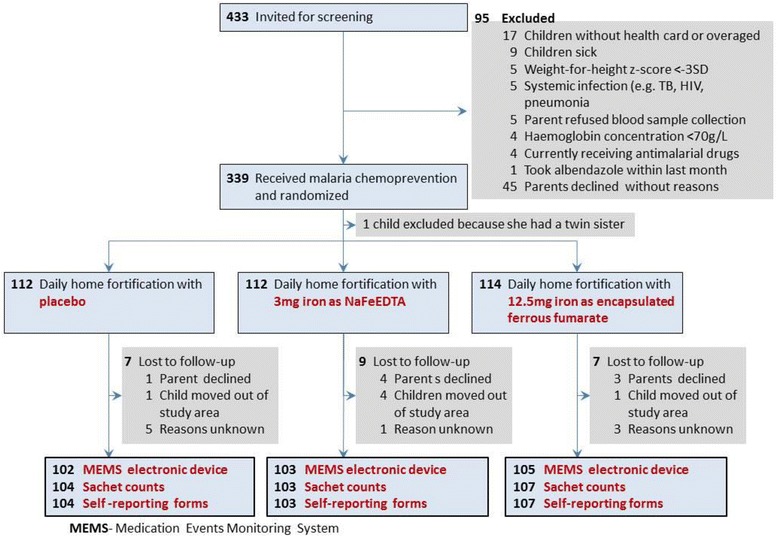
Methods: Three hundred thirty-eight rural Kenyan children aged 12-36 months were randomly allocated to three treatment arms (home fortification with two different iron formulations or placebo). Home fortificants were administered daily by parents or guardians over a 30 day-intervention period. We assessed adherence using an electronic device that stores and provides information of the time and day of opening of the container that was used to store the fortificants sachets in each child's residence. In addition, we assessed adherence by self-reporting and sachet counts. We also measured haemoglobin concentration at the end of intervention.
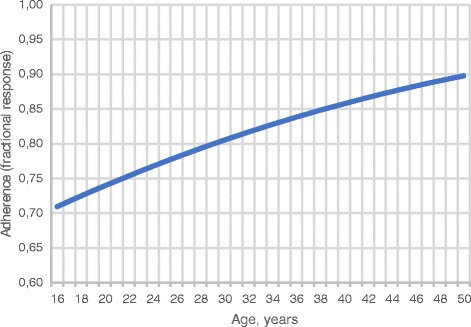
Results: Adherence, defined as having received at least 24 sachets (≥ 80%), during the 30-day intervention period was attained by only 60.6% of children as assessed by the electronic device. The corresponding values were higher when adherence was assessed by self-report (83.9%; difference: 23.3%, 95% CI: 18.8% to 27.8%) or sachet count (86.3%; difference: 25.7%, 95% CI: 21.0% to 30.4%). Among children who received iron, each 10 openings of the electronic cap of the sachet storage container were associated with an increase in haemoglobin concentration at the end of intervention by 1.2 g/L (95% CI: 0.0 to 1.9 g/L). Adherence was associated with the age of the parent but not with intervention group; with age, sex or anthropometric indices of the child; or with age or sex of the parent or guardian.
Conclusions: The use of self -reporting and sachet count may lead to overestimates of adherence to home fortification.
Trial registration: The trial was registered with ClinicalTrials.gov ( NCT02073149 ) on 25 February 2014.
Keywords: Child; Food, fortified; Iron; Kenya; Patient compliance; Preschool; Self-report.
Conflict of interest statement
Ethics approval and consent to participate
Ethical clearance was obtained from the London School of Hygiene and Tropical Medicine Ethical Committee, UK (reference 6503) and the Kenyatta National Hospital Ethical Review Committee, Kenya (reference KNH-ERC/A/402). Either parents or a primary guardian signed the consent forms.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Use of multiple micronutrient powders for home fortification of foods consumed by infants and children 6–23 months of age. Geneva, Switzerland: World Health Organization; 2011. http://apps.who.int/iris/bitstream/10665/44651/1/9789241502047_eng.pdf. Accessed 25 Sept 2017. - PubMed
-
- De-Regil LM, Suchdev PS, Vist GE, Walleser S, Peña-Rosas JP. Home fortification of foods with multiple micronutrient powders for health and nutrition in children under two years of age. Cochrane Database Syst Rev. 2011;9:CD008959. - PubMed
-
- Teshome EM, Andango PEA, Osoti V, Terwel SR, Otieno W, Demir AY, Prentice AM, Verhoef H. Daily home fortification with iron as ferrous fumarate versus NaFeEDTA: a randomised, placebo-controlled, non-inferiority trial in Kenyan children. BMC Med. 2017;15:89. doi: 10.1186/s12916-017-0839-z. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
