

Socioeconomic differences in hearing among middle-aged and older adults: cross-sectional analyses using the Health Survey for England
- PMID: 29391384
- PMCID: PMC5829909
- DOI: 10.1136/bmjopen-2017-019615
Socioeconomic differences in hearing among middle-aged and older adults: cross-sectional analyses using the Health Survey for England
Abstract
Background: Hearing loss impacts on cognitive, social and physical functioning. Both hearing loss and hearing aid use vary across population subgroups. We examined whether hearing loss, and reported current hearing aid use among persons with hearing loss, were associated with different markers of socioeconomic status (SES) in a nationally representative sample of community-dwelling middle-aged and older adults.
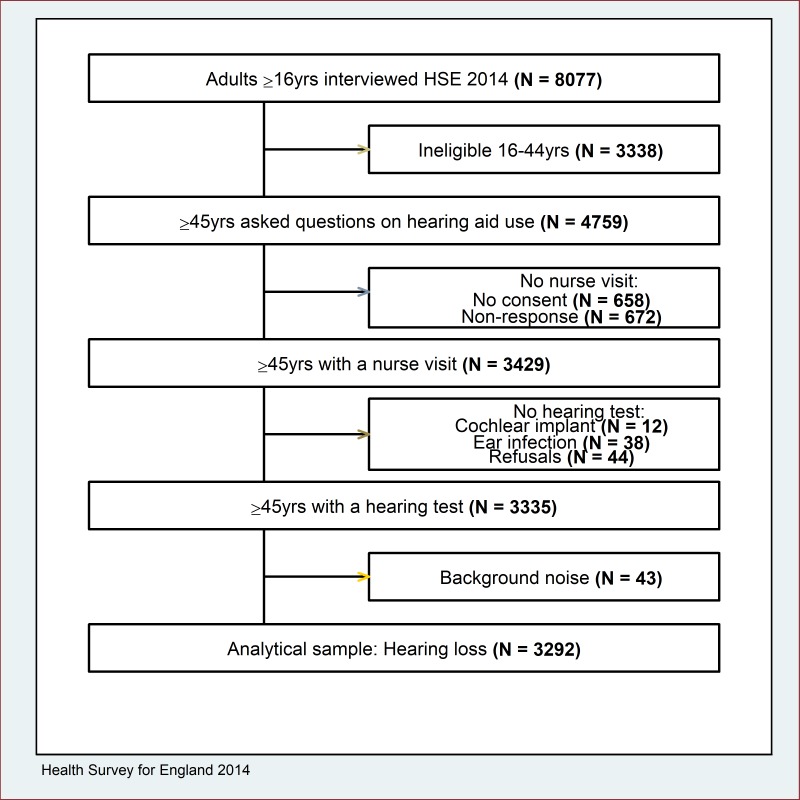
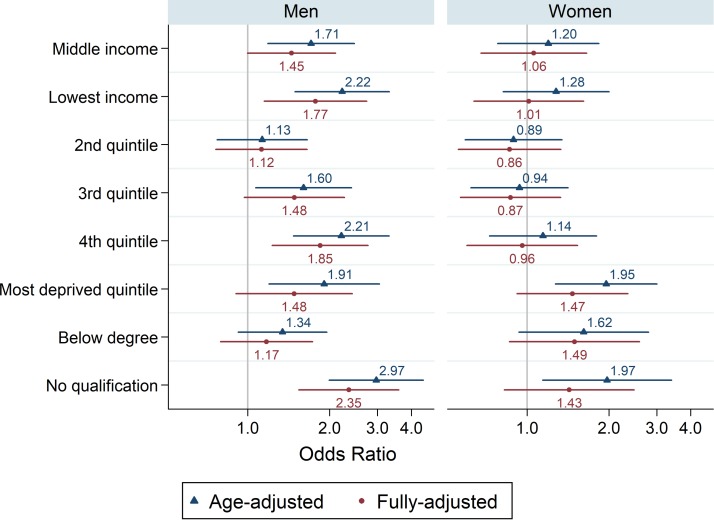
Methods: Hearing was measured using an audiometric screening device in the Health Survey for England 2014 (3292 participants aged 45 years and over). Hearing loss was defined as >35 dB HL at 3.0 kHz in the better-hearing ear. Using sex-specific logistic regression modelling, we evaluated the associations between SES and hearing after adjustment for potential confounders.
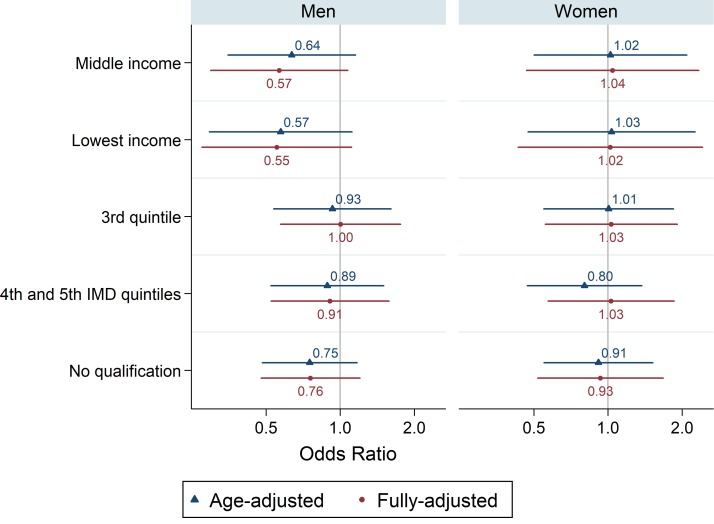
Results: 26% of men and 20% of women aged 45 years and over had hearing loss. Hearing loss was higher among men in the lowest SES groups. For example, the multivariable-adjusted odds of hearing loss were almost two times as high for those in the lowest versus the highest income tertile (OR 1.77, 95% CI 1.15 to 2.74). Among those with hearing loss, 30% of men and 27% of women were currently using a hearing aid. Compared with men in the highest income tertile, the multivariable-adjusted odds of using a hearing aid nowadays were lower for men in the middle (OR 0.50, 95% CI 0.25 to 0.99) and the lowest (OR 0.47, 95% CI 0.23 to 0.97) income tertiles. Associations between SES and hearing were weaker or null among women.
Conclusions: While the burden of hearing loss fell highest among men in the lowest SES groups, current hearing aid use was demonstrably lower. Initiatives to detect hearing loss early and increase the uptake and the use of hearing aids may provide substantial public health benefits and reduce socioeconomic inequalities in health.
Keywords: epidemiology; hearing aids; hearing loss; social inequalities; surveys.
© Article author(s) (or their employer(s) unless otherwise stated in the text of the article) 2018. All rights reserved. No commercial use is permitted unless otherwise expressly granted.
Conflict of interest statement
Competing interests: None declared.
Figures
References
-
- World Health Organization. Prevention of noise-induced hearing loss. Geneva, Switzerland: World Health Organization, 1997.
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous