

Efficacy of supervised maintenance exercise following pulmonary rehabilitation on health care use: a systematic review and meta-analysis
- PMID: 29391784
- PMCID: PMC5768431
- DOI: 10.2147/COPD.S150650
Efficacy of supervised maintenance exercise following pulmonary rehabilitation on health care use: a systematic review and meta-analysis
Abstract
Introduction: The clinical benefit of continued supervised maintenance exercise programs following pulmonary rehabilitation in COPD remains unclear. This systematic review aimed to synthesize the available evidence on the efficacy of supervised maintenance exercise programs compared to usual care following pulmonary rehabilitation completion on health care use and mortality.
Methods: Electronic databases (MEDLINE, Embase, CINAHL, Cochrane Central Register of Controlled Trials, Web of Science, and PEDro) and trial registers (ClinicalTrials.gov and Current Controlled Trials) were searched for randomized trials comparing supervised maintenance exercise programs with usual care following pulmonary rehabilitation completion. Primary outcomes were respiratory-cause hospital admissions, exacerbations requiring treatment with antibiotics and/or systemic corticosteroids, and mortality.
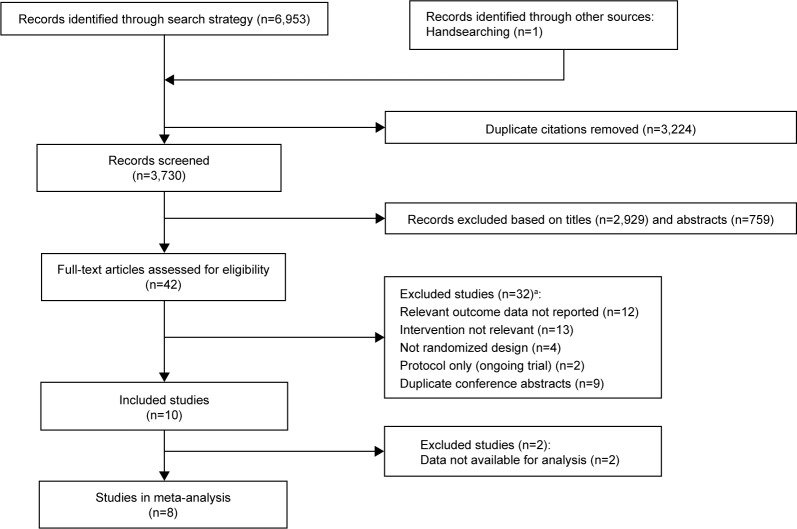
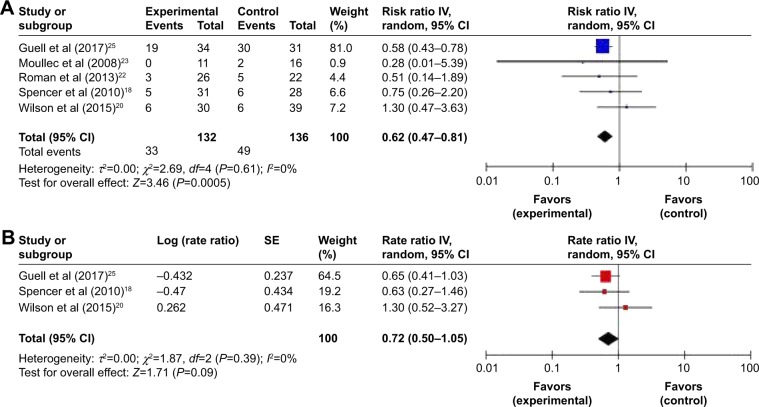
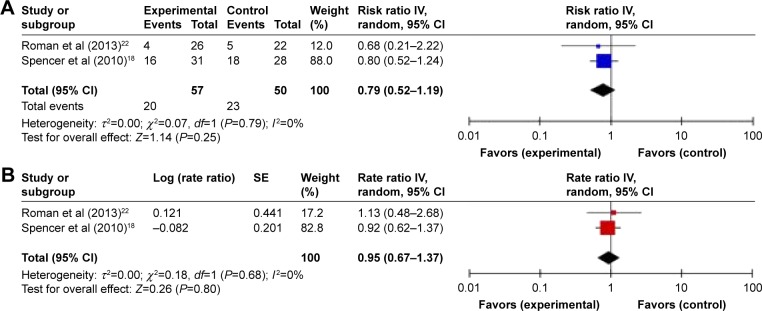
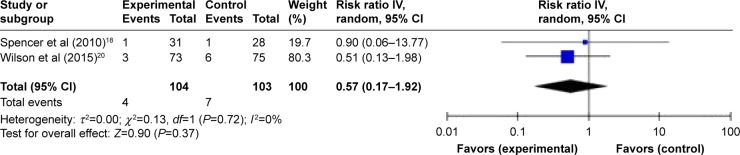
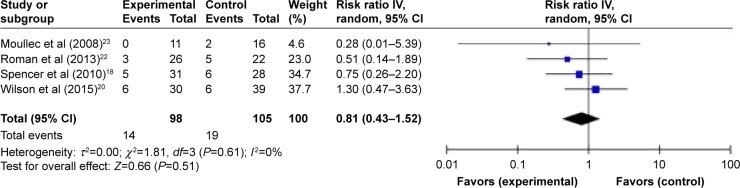
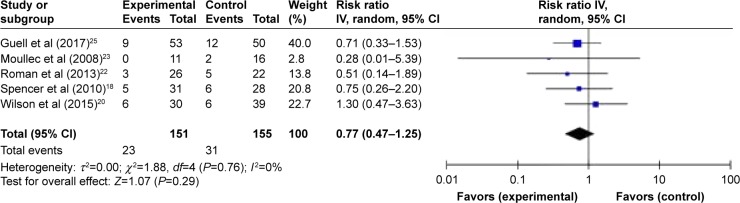
Results: Eight trials (790 COPD patients) met the inclusion criteria, six providing data for meta-analysis. Continued supervised maintenance exercise compared to usual care following pulmonary rehabilitation completion significantly reduced the risk of experiencing at least one respiratory-cause hospital admission (risk ratio 0.62, 95% confidence interval [CI] 0.47-0.81, P<0.001). Meta-analyses also suggested that supervised maintenance exercise leads to a clinically important reduction in the rate of respiratory-cause hospital admissions (rate ratio 0.72, 95% CI 0.50-1.05, P=0.09), overall risk of an exacerbation (risk ratio 0.79, 95% CI 0.52-1.19, P=0.25), and mortality (risk ratio 0.57, 95% CI 0.17-1.92, P=0.37).
Conclusion: In the first systematic review of the area, current evidence demonstrates that continued supervised maintenance exercise compared to usual care following pulmonary rehabilitation reduces health care use in COPD. The variance in the quality of the evidence included in this review highlights the need for this evidence to be followed up with further high-quality randomized trials.
Keywords: exacerbations; health outcomes; hospitalization; pulmonary rehabilitation; supervised maintenance programs.
Conflict of interest statement
Disclosure The authors report no conflicts of interest in this work.
Figures
References
-
- Andrews SM, Carter M, Deoghare H, Mills PK, van Gundy K, Jain VV. Pulmonary rehabilitation maintenance program prevents accelerated FEV1 decline and may prevent exacerbations in patients with severe COPD. Am J Respir Crit Care Med. 2015;191:A2013.
-
- Berry MJ, Rejeski WJ, Adair NE, Ettinger WH, Zaccaro DJ, Sevick MA. A randomized, trolled trial comparing long-term and short-term exercise in patients with chronic obstructive pulmonary disease. J Cardiopulm Rehabil. 2003;23:60–68. - PubMed
-
- Bertolini GN, Ramos D, Leite MR, et al. Effects of a home-based exercise program after supervised resistance training in patients with chronic obstructive pulmonary disease. Medicina. 2016;49:331–337.
-
- Brooks D, Krip B, Mangovski-Alzamora S, Goldstein RS. The effect of postrehabilitation programmes among individuals with chronic obstructive pulmonary disease. Eur Respir J. 2002;20:20–29. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
