

Increased Small Intestinal Permeability during Severe Acute Exacerbations of COPD
- PMID: 29393240
- PMCID: PMC5985742
- DOI: 10.1159/000485935
Increased Small Intestinal Permeability during Severe Acute Exacerbations of COPD
Abstract
Background: Disturbances of intestinal integrity, manifested by increased gastro-intestinal (GI) permeability, have been found in chronic obstructive pulmonary disease (COPD) patients during physical activity, often associated with intermittent hypoxic periods. Evidence about extrapulmonary organ disturbances, especially of the GI tract, during hospitalised acute exacerbation of COPD (AE-COPD) with hypoxaemic respiratory failure (RF) is lacking.
Objective: The aim was to assess changes in GI permeability in patients with AE-COPD and during recovery 4 weeks later.
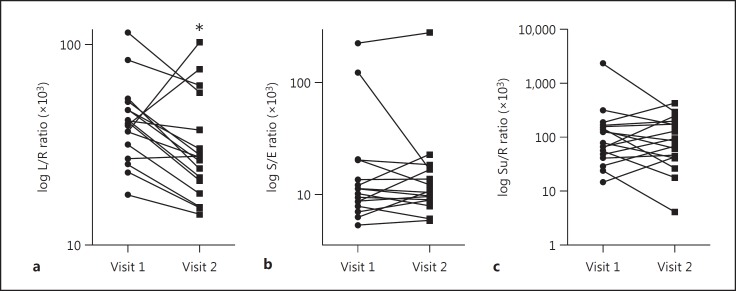
Methods: All patients admitted to our hospital with AE-COPD accompanied by hypoxaemia at admission (PaO2 <8.7 kPa or O2 saturation <93%) were screened between October 2013 and February 2014. Patients with a history of GI or renal disease, chronic heart failure, or use of non-steroidal anti-inflammatory drugs in the 48 h before the test were excluded. GI permeability was assessed by evaluating urinary excretion ratios of the orally ingested sugars lactulose/L-rhamnose (L/R ratio), sucrose/L-rhamnose (Su/R ratio) and sucralose/erythritol (S/E ratio).
Results: Seventeen patients with severe to very severe COPD completed the study. L/R ratio (×103) at admission of AE-COPD was significantly higher than in the recovery condition (40.9 [29.4-49.6] vs. 27.3 [19.5-47.7], p = 0.039), indicating increased small intestinal permeability. There were no significant differences in the individual sugar levels in urine nor in the 0- to 5-h urinary S/E and Su/R ratios between the 2 visits.
Conclusion: This is the first study showing increased GI permeability during hospitalised AE-COPD accompanied by hypoxaemic RF. Therefore, GI integrity in COPD patients is an attractive target for future research and for the development of interventions to alleviate the consequences of AE-COPD.
Keywords: Barrier function; Hospital admission; Hypoxaemia; Lactulose/L-rhamnose ratio; Small intestine.
© 2018 The Author(s) Published by S. Karger AG, Basel.
Figures
References
-
- van Eeden SF, Sin DD. Chronic obstructive pulmonary disease: a chronic systemic inflammatory disease. Respiration. 2008;75:224–238. - PubMed
-
- Pauwels RA, Buist AS, Calverley PM, Jenkins CR, Hurd SS, Committee GS. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease. NHLBI/WHO Global Initiative for Chronic Obstructive Lung Disease (GOLD) Workshop summary. Am J Respir Crit Care Med. 2001;163:1256–1276. - PubMed
-
- Celli BR. MacNee W; ATS/ERS Task Force: Standards for the diagnosis and treatment of patients with COPD: a summary of the ATS/ERS position paper. Eur Respir J. 2004;23:932–946. - PubMed
-
- John BA, Wood SG, Hawkins DR. The pharmacokinetics and metabolism of sucralose in the mouse. Food Chem Toxicol. 2000;38((suppl 2)):S107–S110. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
