

The effect of an intraoperative, lung-protective ventilation strategy in neurosurgical patients undergoing craniotomy: study protocol for a randomized controlled trial
- PMID: 29394907
- PMCID: PMC5797412
- DOI: 10.1186/s13063-018-2447-4
The effect of an intraoperative, lung-protective ventilation strategy in neurosurgical patients undergoing craniotomy: study protocol for a randomized controlled trial
Abstract
Background: Ventilator-induced lung injury is a major cause of postoperative pulmonary complications (PPCs) in patients undergoing neurosurgery after general anesthesia. However, there is no study on the effect of a lung-protective ventilation strategy in patients undergoing neurosurgery.
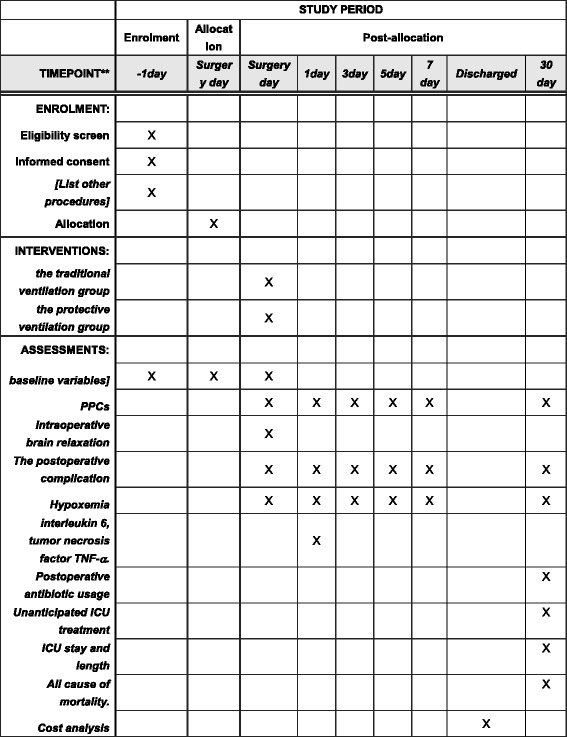
Methods: This is a single-center, randomized, parallel-group controlled trial which will be carried out at Beijing Tiantan Hospital, Capital Medical University. Three hundred and thirty-four patients undergoing intracranial tumor surgery will be randomly allocated to the control group and the protective-ventilation strategy group. In the control group, tidal volume (VT) will be set at 10-12 ml/kg of predicted body weight but PEEP and recruitment maneuvers will not be used. In the protective group, VT will be set at 6-8 ml/kg of predicted body weight, PEEP at 6-8 cmH2O, and a recruitment maneuver will be used intermittently. The primary outcome is pulmonary complications within 7 days postoperatively. Secondary outcomes include intraoperative brain relaxation, the postoperative complications within 30 days and the cost analysis.
Discussion: This study aims to determine if the protective, pulmonary-ventilation strategy decreases the incidence of PPCs in patients undergoing neurosurgical anesthesia. If our results are positive, the study will indicate whether the protective, pulmonary-ventilation strategy is efficiently and safely used in neurosurgical patients undergoing the craniotomy.
Trial registration: ClinicalTrials.gov, ID: NCT02386683 . Registered on 18 October 2014.
Keywords: Brain relaxation; Craniotomy; Lung protection; Postoperative pulmonary complications; Randomized controlled trial.
Conflict of interest statement
Ethics approval and consent to participate
The trial will be conducted by the ethical principles outlined in the Declaration of Helsinki, 1996 [14]; National Ethics Review for Biomedical Research Involving Humans (Trial), 2007 [15]; and International Ethical Guidelines for Biomedical Research Involving Human Subjects, 2002 [16]. Approval was obtained from the Ethics Committee of Beijing Tiantan Hospital on 18 October 2014 (reference number KY-2014-031-02).
Consent for publication
Not applicable
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Fernandez-Bustamante A, Frendl G, Sprung J, Subramaniam B, Martinez Ruiz R, Lee JW, Henderson WG, Moss A, Mehdiratta N, Colwell MM, Bartels K, Kolodzie K, Giquel J, Vidal Melo MF. Postoperative pulmonary complications, early mortality, and hospital stay following noncardiothoracic surgery: a multicenter study by the perioperative research network investigators. JAMA Surg. 2017;152(2):157–66. doi: 10.1001/jamasurg.2016.4065. - DOI - PMC - PubMed
-
- Arozullah AM, Daley J, Henderson WG, Khuri SF. Multifactorial risk index for predicting postoperative respiratory failure in men after major noncardiac surgery: the National Veterans Administration Surgical Quality Improvement Program. Ann Surg. 2000;232:242–53. doi: 10.1097/00000658-200008000-00015. - DOI - PMC - PubMed
-
- Shander A, Fleisher LA, Barie PS, Bigatello LM, Sladen RN, Watson CB. Clinical and economic burden of postoperative pulmonary complications: patient safety summit on definition, risk-reducing interventions, and preventive strategies. Crit Care Med. 2011;39:2163–72. doi: 10.1097/CCM.0b013e31821f0522. - DOI - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
