

Quantification of cancer risk in glomerulonephritis
- PMID: 29394927
- PMCID: PMC5797419
- DOI: 10.1186/s12882-018-0828-2
Quantification of cancer risk in glomerulonephritis
Abstract
Background: The association of increased cancer risk with glomerulonephritis (GN) is well known, but controversy exists concerning which types of GN are involved, and the size of the association. A national registry survey was performed to assess the size of this association, and the temporal relationship of cancer diagnosis to GN diagnosis.
Methods: All patients with biopsy-proven GN between 1985 and 2015 in Denmark were extracted from The Danish Renal Biopsy Registry and the National Pathology Data Bank. Incident cancer diagnoses between 10 years previous and 10 years subsequent to the GN diagnosis were extracted from the Danish Cancer Registry. Residence, birth and death data were obtained from the National Patient Register. Expected cancer incidence, classified according to cohort, age and sex were extracted from the Nordcan database.
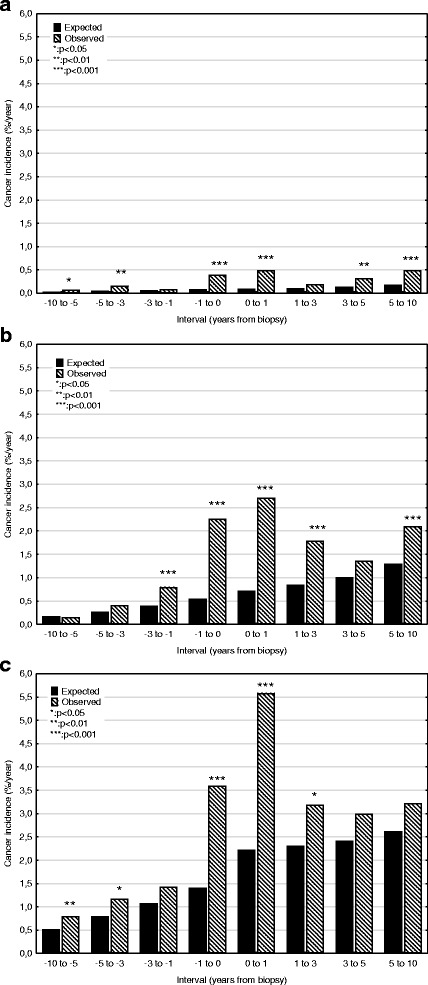
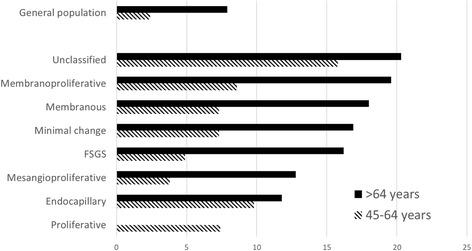
Results: Nine hundred eleven cancers were diagnosed in 5594 patients. Thirty five percent were prevalent at renal biopsy. Prevalence at biopsy was 5.5% (expected 3.1%), but incidence was not increased < 1 year before biopsy. Increased cancer rates were seen for GN forms: minimal change, endocapillary, focal segmental glomerulosclerosis, mesangioproliferative, membranous, focal segmental, membranoproliferative, proliferative, ANCA-associated vasculitis, lupus nephritis and unclassified. Increased cancer rates were seen for lung, prostate, renal, non-Hodgkin lymphoma, myeloma, leukaemia and skin. The increased incidence was mainly limited to - 1 to 1 year after biopsy, but skin cancer showed an increased risk over time. Some diagnoses showed an increase 5-10 years after biopsy. Incidence was raised for patients with uraemia and nephrosis, but less for proteinuria or haematuria. Cancers in patients < 45 years were rare. The risk of developing cancer 0-3 years after biopsy for patients 45-64 years varied from 7.3% (minimal change) to 15.8% (unclassified GN); > 64 years from 11.8 (endocapillary GN) to 20.3% (unclassified). The diagnosis with the highest risk was membranoproliferative GN (8.6 & 19.6%).
Conclusions: Cancer rates are increased for many cancer and most GN diagnoses. Cancer screening for patients < 45 years and for patients without nephrosis or uraemia may not be necessary. The findings suggest that screening programs for specific GN diagnoses can be extended to other GN forms.
Keywords: Cancer; Epidemiology; Glomerulonephritis; Haematuria; Nephrotic syndrome; Proteinuria; Uraemia.
Conflict of interest statement
Ethics approval and consent to participate
The project was approved by the Danish Data Protection Agency (REG-132-2015), and by the Danish Patient Safety Authority (3–3013-1440/1). Due to the anonymized, non-invasive, retrospective nature of the study, the requirement for specific scientific ethical committee was waived by the Danish Patient Safety Authority.
Consent for publication
Due to the anonymized, non-invasive, retrospective nature of the study, the Danish Patient Safety Authority (3–3013-1440/1) has waved the requirement for individual patient approval.
Competing interests
The authors have no conflict of interest. The results presented in this paper have not been published previously in whole or part, except in abstract format.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures


References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
