

Windkessel model of hemodynamic state supported by a pulsatile ventricular assist device in premature ventricle contraction
- PMID: 29394944
- PMCID: PMC5797383
- DOI: 10.1186/s12938-018-0440-5
Windkessel model of hemodynamic state supported by a pulsatile ventricular assist device in premature ventricle contraction
Abstract
Background: Counter-pulsation control (CPC) by ventricular assist devices (VADs) is believed to reduce cardiac load and increase coronary perfusion. However, patients with VADs have a higher risk of arrhythmia, which may cause the CPC to fail. Consequently, CPC has not been applied by VADs in clinical practice. The phase-locked loop (PLL) algorithm for CPC is readily implemented in VADs; however, it requires a normal, consistent heartbeat for adequate performance. When an arrhythmia occurs, the algorithm maintains a constant pumping rate despite the unstable heartbeat. Therefore, to apply the PLL algorithm to CPC, the hemodynamic effects of abnormal heartbeats must be analyzed.
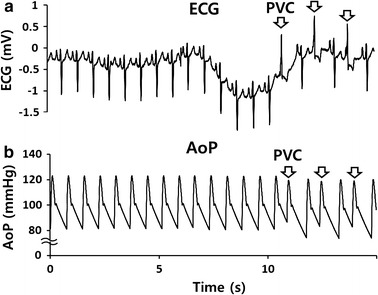
Objectives: This study sought to predict the hemodynamic effects in patients undergoing CPC using VADs, based on electrocardiogram (ECG) data, including a wide range of heart rate (HR) changes caused by premature ventricular contraction (PVC) or other reasons.
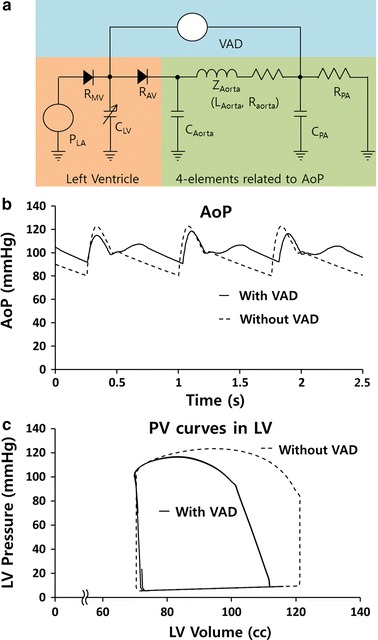
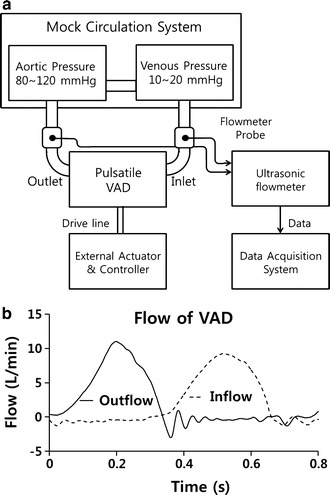
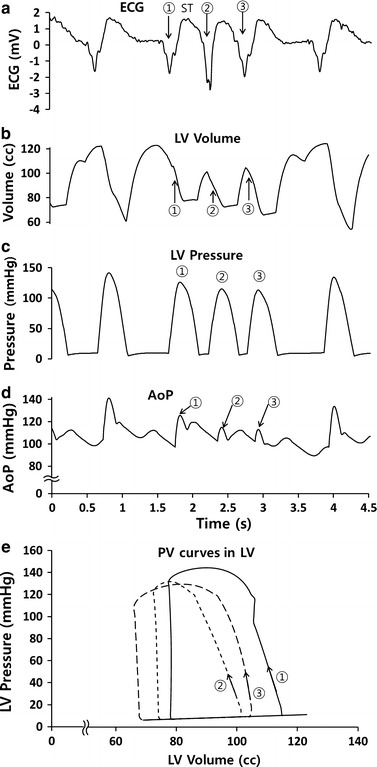
Methods: A four-element Windkessel hemodynamic model was used to reproduce the patient's aortic blood pressure in this study. ECG data from 15 patients with severe congestive heart failure were used to assess the effect of the CPC on the patients' hemodynamic state. The input and output flow characteristics of the pulsatile VAD (LibraHeart I, Cervika, Korea) were measured using an ultrasound blood flow meter (TS410, Transonic, USA), with the aortic pressure maintained at 80-120 mmHg. All other patient conditions were also reproduced.
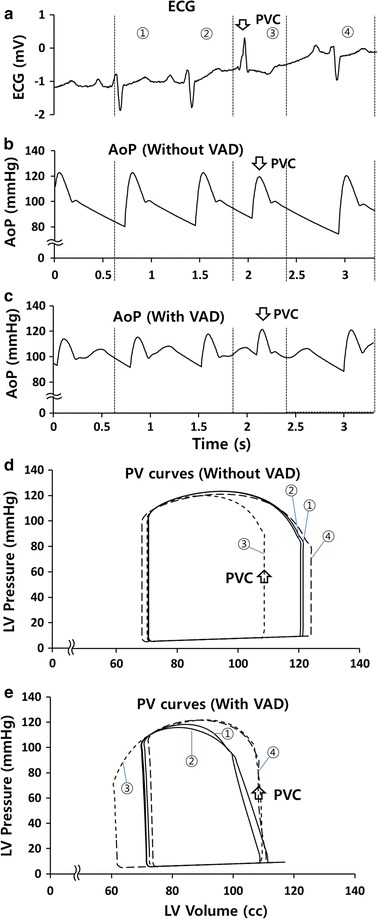
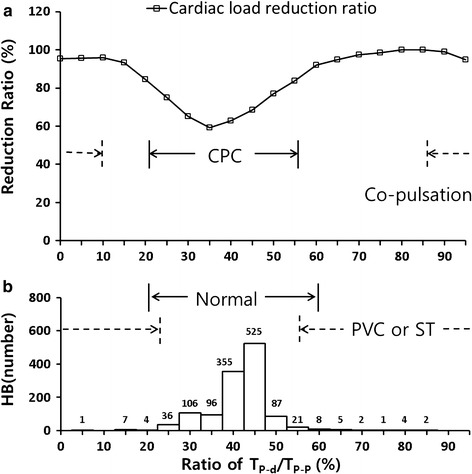
Results: In patients with PVCs or normal heartbeats, CPC controlled by a VAD reduced the cardiac load by 20 and 40%, respectively. When the HR was greater for other reasons, such as sinus tachycardia, simultaneous ejection from the heart and VAD was observed; however, the cardiac load was not increased by rapid cardiac contractions resulting from decreased left ventricle volume. These data suggest that the PLL algorithm reduces the cardiac load and maintains consistent hemodynamic changes.
Keywords: Arrhythmia; Counter-pulsation control; Phase-locked loop; Pulsatile ventricular assist device; Windkessel model.
Figures

References
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
