

Rationale and design of the Clinical and Histologic Analysis of Mesenchymal Stromal Cells in AmPutations (CHAMP) trial investigating the therapeutic mechanism of mesenchymal stromal cells in the treatment of critical limb ischemia
- PMID: 29395424
- PMCID: PMC6019117
- DOI: 10.1016/j.jvs.2017.09.057
Rationale and design of the Clinical and Histologic Analysis of Mesenchymal Stromal Cells in AmPutations (CHAMP) trial investigating the therapeutic mechanism of mesenchymal stromal cells in the treatment of critical limb ischemia
Abstract
Objective: Currently, there are no accepted nonsurgical therapies that improve the delivery of blood-derived nutrients to patients with critical limb ischemia. Here, we describe the ongoing phase 1/2 Clinical and Histologic Analysis of Mesenchymal Stromal Cells in AmPutations (CHAMP) trial, which will provide crucial evidence of the safety profile of mesenchymal stromal cells (MSCs) and explore their therapeutic mechanisms in the setting of critical limb ischemia requiring below-knee amputation (BKA).
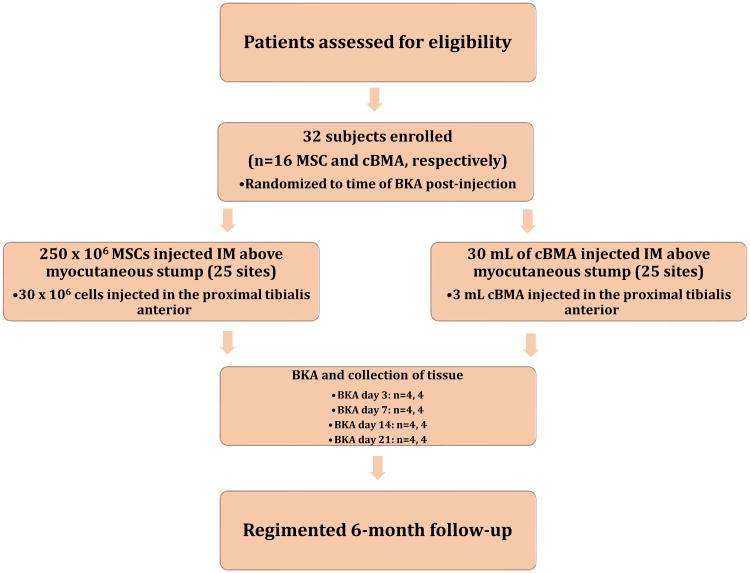
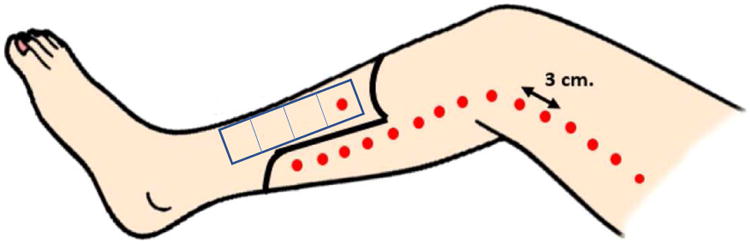
Methods: In the CHAMP and the parallel marrowCHAMP trials (hereafter grouped together as CHAMP), a total of 32 extremities with rest pain or tissue loss requiring BKA will be enrolled to receive intramuscular injections of allogeneic MSCs (CHAMP; n = 16) or autogenous concentrated bone marrow aspirate (marrowCHAMP; n = 16) along the distribution of the BKA myocutaneous flap and proximal tibialis anterior. After treatment, subjects are randomized to BKA at four time points after injection (days 3, 7, 14, and 21). At the time of amputation, skeletal muscle is collected at 2-cm increments from the tibialis injection site and used to determine proangiogenic cytokine description, MSC retention, quantification of proangiogenic hematopoietic progenitor cells, and histologic description. Clinical limb perfusion before and after treatment will be quantified using transcutaneous oximetry, toe-brachial index, ankle-brachial index, and indocyanine angiography. Additional clinical end points include all-cause mortality, need for amputation revision, and gangrene incidence during the 6-month post-treatment follow-up.
Results: Enrollment is under way, with 10 patients treated per protocol thus far. We anticipate full conclusion of follow-up within the next 24 months.
Conclusions: CHAMP will be pivotal in characterizing the safety, efficacy, and, most important, therapeutic mechanism of allogeneic MSCs and autogenous concentrated bone marrow aspirate in ischemic skeletal muscle.
Trial registration: ClinicalTrials.gov NCT02685098.
Copyright © 2017 Society for Vascular Surgery. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Norgren L, Hiatt W, Dormandy J, Nehler M, Harris K, Fowkes F, et al. Inter-society consensus for the management of peripheral arterial disease. J Vasc Surg. 2007 - PubMed
-
- Tateishi-Yuyama E, Matsubara H, Murohara T, Ikeda U, Shintani S, Masaki H, et al. Therapeutic angiogenesis for patients with limb ischaemia by autologous transplantation of bone-marrow cells: a pilot study and a randomised controlled trial. Lancet. 2002 0140-6736 (Print) - PubMed
-
- Wang SK, Green LA, Motaganahalli RL, Wilson MG, Fajardo A, Murphy MP. Rationale and Design of the MOBILE Trial Investigating Autologous Bone Marrow Cell Therapy for Critical Limb Ischemia (In Press) Journal of vascular surgery. 2017 - PubMed
-
- Liang TW, Jester A, Motaganahalli RL, Wilson MG, G'Sell P, Akingba GA, et al. Autologous bone marrow mononuclear cell therapy for critical limb ischemia is effective and durable. Journal of vascular surgery. 2016;63(6):1541–1545. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
