

A New Diagnostic Approach to the Adult Patient with Acute Dizziness
- PMID: 29395695
- PMCID: PMC6049818
- DOI: 10.1016/j.jemermed.2017.12.024
A New Diagnostic Approach to the Adult Patient with Acute Dizziness
Abstract
Background: Dizziness, a common chief complaint, has an extensive differential diagnosis that includes both benign and serious conditions. Emergency physicians must distinguish the majority of patients with self-limiting conditions from those with serious illnesses that require acute treatment.
Objective of the review: This article presents a new approach to diagnosis of the acutely dizzy patient that emphasizes different aspects of the history to guide a focused physical examination with the goal of differentiating benign peripheral vestibular conditions from dangerous posterior circulation strokes in the emergency department.
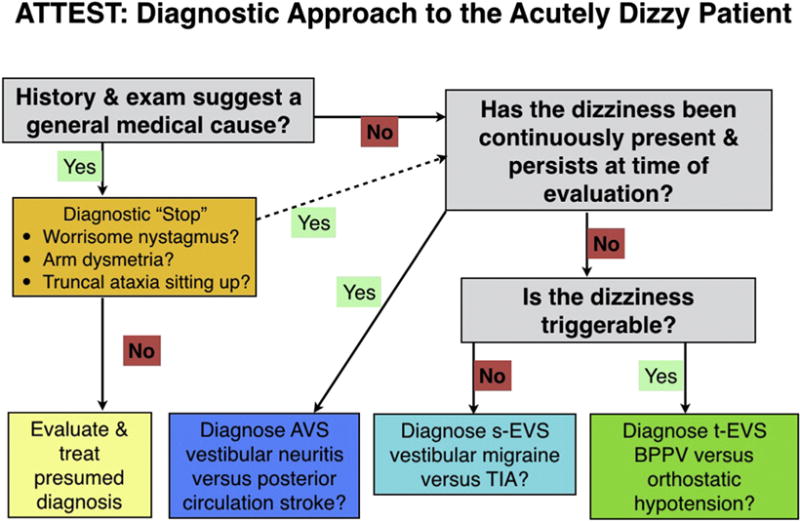
Discussion: Currently, misdiagnoses are frequent and diagnostic testing costs are high. This relates in part to use of an outdated, prevalent, diagnostic paradigm. The traditional approach, which relies on dizziness symptom quality or type (i.e., vertigo, presyncope, or disequilibrium) to guide inquiry, does not distinguish benign from dangerous causes, and is inconsistent with current best evidence. A new approach divides patients into three key categories using timing and triggers, guiding a differential diagnosis and targeted bedside examination protocol: 1) acute vestibular syndrome, where bedside physical examination differentiates vestibular neuritis from stroke; 2) spontaneous episodic vestibular syndrome, where associated symptoms help differentiate vestibular migraine from transient ischemic attack; and 3) triggered episodic vestibular syndrome, where the Dix-Hallpike and supine roll test help differentiate benign paroxysmal positional vertigo from posterior fossa structural lesions.
Conclusions: The timing and triggers diagnostic approach for the acutely dizzy patient derives from current best evidence and offers the potential to reduce misdiagnosis while simultaneously decreases diagnostic test overuse, unnecessary hospitalization, and incorrect treatments.
Keywords: BPPV; diagnosis; dizziness; misdiagnosis; nystagmus; posterior circulation stroke; vertigo; vestibular neuritis.
Copyright © 2017 Elsevier Inc. All rights reserved.
Figures
References
-
- Cheung CS, Mak PS, Manley KV, et al. Predictors of important neurological causes of dizziness among patients presenting to the emergency department. Emerg Med J. 2010;27:517–521. - PubMed
-
- Saber Tehrani AS, Coughlan D, Hsieh YH, et al. Rising annual costs of dizziness presentations to U.S. emergency departments. Acad Emerg Med. 2013;20:689–696. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
