

ISCEV guide to visual electrodiagnostic procedures
- PMID: 29397523
- PMCID: PMC5811581
- DOI: 10.1007/s10633-017-9621-y
ISCEV guide to visual electrodiagnostic procedures
Abstract
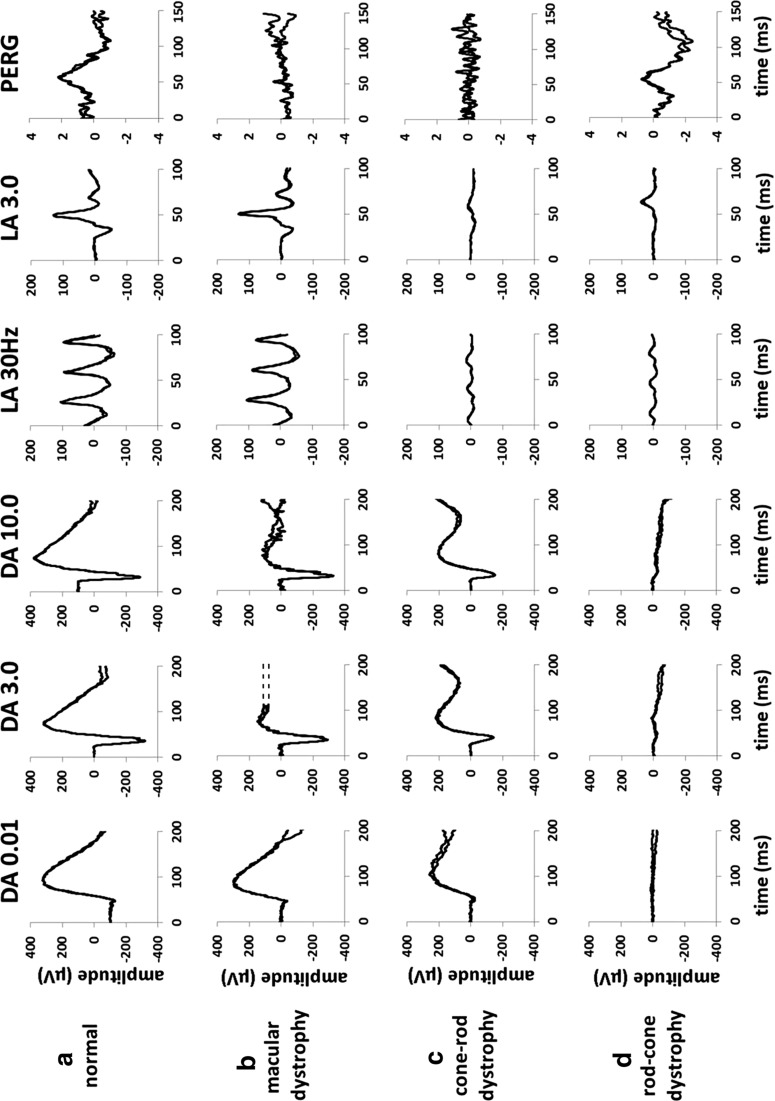
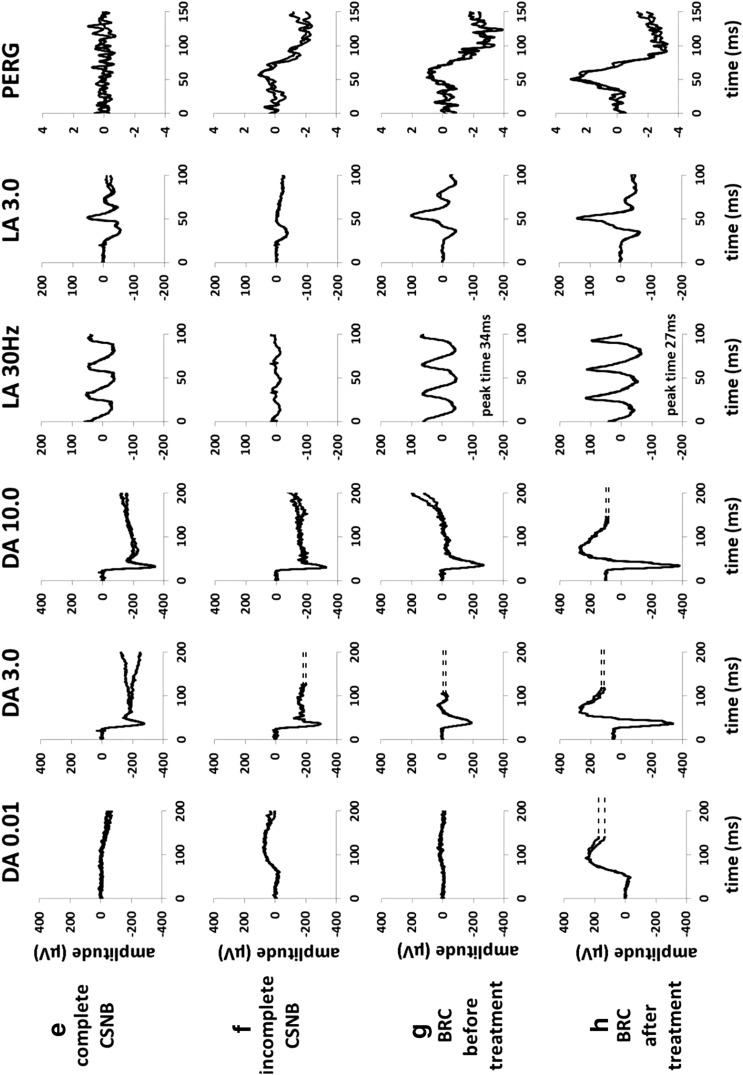
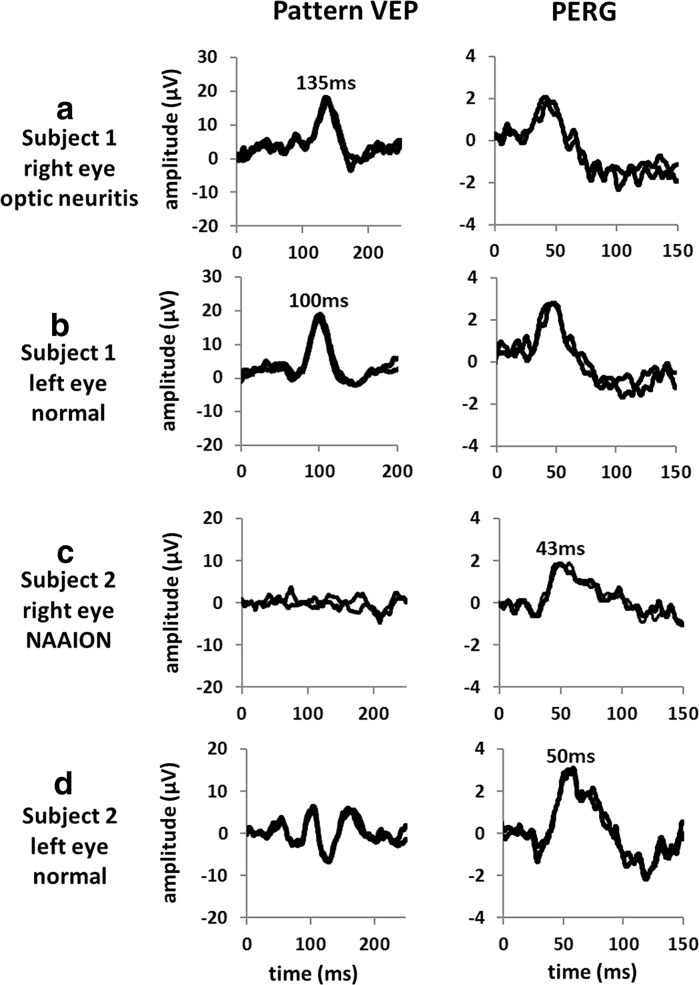
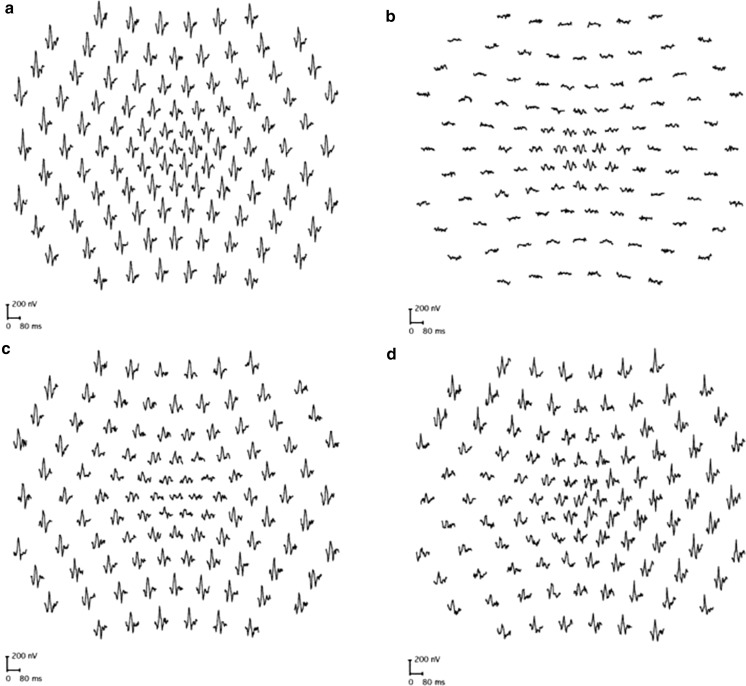
Clinical electrophysiological testing of the visual system incorporates a range of noninvasive tests and provides an objective indication of function relating to different locations and cell types within the visual system. This document developed by the International Society for Clinical Electrophysiology of Vision provides an introduction to standard visual electrodiagnostic procedures in widespread use including the full-field electroretinogram (ERG), the pattern electroretinogram (pattern ERG or PERG), the multifocal electroretinogram (multifocal ERG or mfERG), the electrooculogram (EOG) and the cortical-derived visual evoked potential (VEP). The guideline outlines the basic principles of testing. Common clinical presentations and symptoms are described with illustrative examples and suggested investigation strategies.
Keywords: Clinical electrophysiology; Electrooculogram (EOG); Electroretinogram (ERG); ISCEV standards; Maculopathy; Multifocal ERG (mfERG); Optic neuropathy; Pattern ERG; Retinopathy; Visual evoked potential (VEP).
Conflict of interest statement
Conflict of interest
All authors certify that they have no affiliations with or involvement in any organization or entity with any financial interest (such as honoraria; educational grants; participation in speakers’ bureaus; membership, employment consultancies, stock ownership, or other equity interest; and expert testimony or patent-licensing arrangements) or non-financial interest (such as personal or professional relationships, affiliations, knowledge or beliefs) in the subject matter or materials discussed in this manuscript.
Informed consent
For this type of study formal consent is not required.
Statement of human rights
This article does not contain any research studies with human participants performed by any of the authors.
Statement on the welfare of animals
This article does not contain any research studies with animals performed by any of the authors.
Figures

References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
