

Markers of early progressive renal decline in type 2 diabetes suggest different implications for etiological studies and prognostic tests development
- PMID: 29398132
- PMCID: PMC5911430
- DOI: 10.1016/j.kint.2017.11.024
Markers of early progressive renal decline in type 2 diabetes suggest different implications for etiological studies and prognostic tests development
Abstract
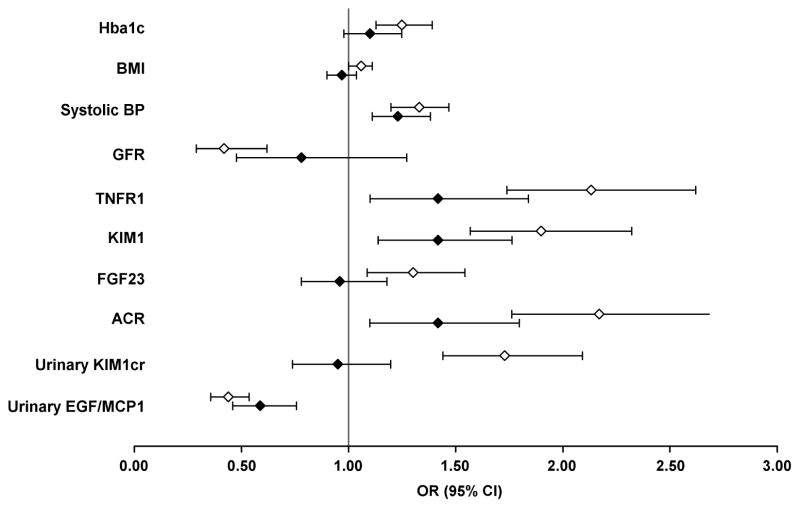
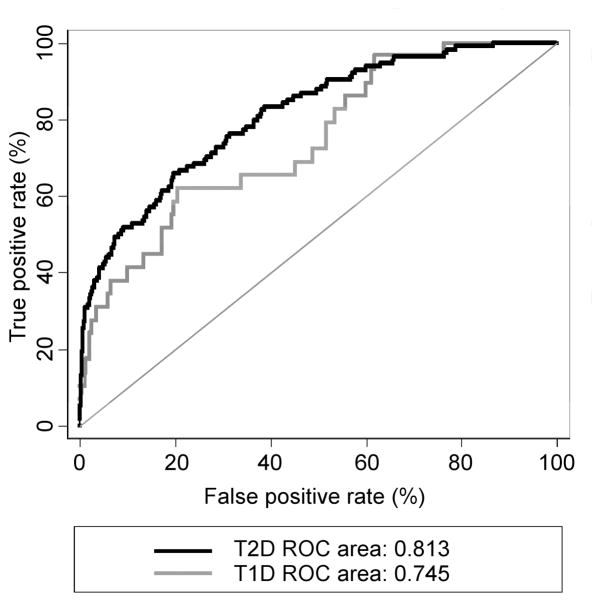
To identify determinants of early progressive renal decline in type 2 diabetes a range of markers was studied in 1032 patients enrolled into the 2nd Joslin Kidney Study. eGFR slopes estimated from serial measurements of serum creatinine during 5-12 years of follow-up were used to define early renal decline. At enrollment, all patients had normal eGFR, 58% had normoalbuminuria and 42% had albuminuria. Early renal decline developed in 6% and in 18% patients, respectively. As determinants, we examined baseline values of clinical characteristics, circulating markers: TNFR1, KIM-1, and FGF23, and urinary markers: albumin, KIM-1, NGAL, MCP-1, EGF (all normalized to urinary creatinine) and the ratio of EGF to MCP-1. In univariate analysis, all plasma and urinary markers were significantly associated with risk of early renal decline. When analyzed together, systolic blood pressure, TNFR1, KIM-1, the albumin to creatinine ratio, and the EGF/MCP-1 ratio remained significant with the latter having the strongest effect. Integration of these markers into a multi-marker prognostic test resulted in a significant improvement of discriminatory performance of risk prediction of early renal decline, compared with the albumin to creatinine ratio and systolic blood pressure alone. However, the positive predictive value was only 50% in albuminuric patients. Thus, markers in plasma and urine indicate that the early progressive renal decline in Type 2 diabetes has multiple determinants with strong evidence for involvement of tubular damage. However, new, more informative markers are needed to develop a better prognostic test for such decline that can be used in a clinical setting.
Keywords: diabetes; diabetic nephropathy; microalbuminuria.
Copyright © 2017 International Society of Nephrology. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Collins AJ, Foley RN, Herzog C, Chavers B, Gilbertson D, Ishani A. US renal data system 2010 annual data report. Am J Kidney Dis. 2011;57(Suppl 1):A8-e1–526. - PubMed
-
- Thomas MC, Cooper ME, Zimmet P. Changing epidemiology of type 2 diabetes mellitus and associated chronic kidney disease. Nature Reviews Nephrology. 2016;12:73–81. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
