

Kidney disease in the setting of HIV infection: conclusions from a Kidney Disease: Improving Global Outcomes (KDIGO) Controversies Conference
- PMID: 29398134
- PMCID: PMC5983378
- DOI: 10.1016/j.kint.2017.11.007
Kidney disease in the setting of HIV infection: conclusions from a Kidney Disease: Improving Global Outcomes (KDIGO) Controversies Conference
Abstract
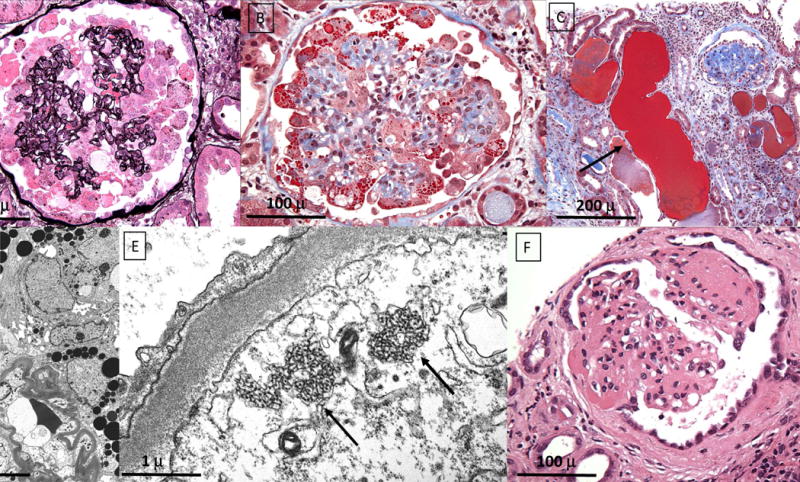
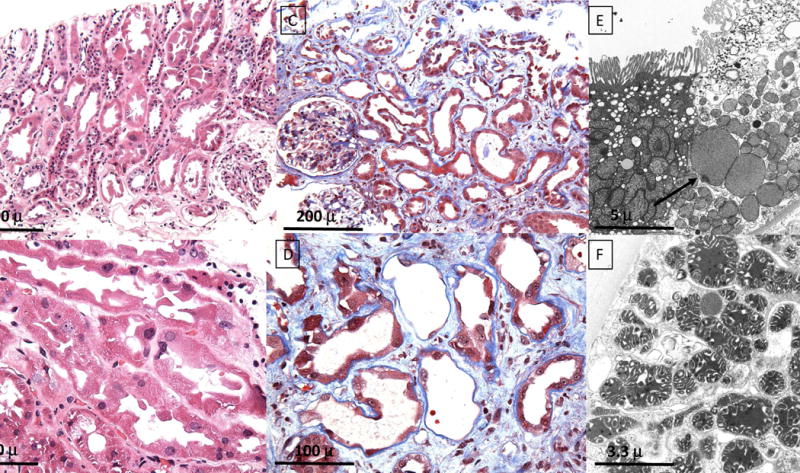
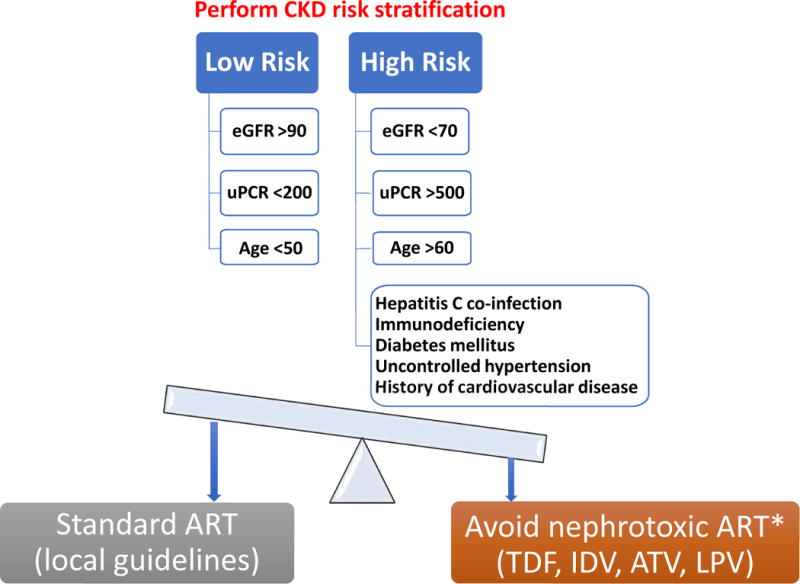
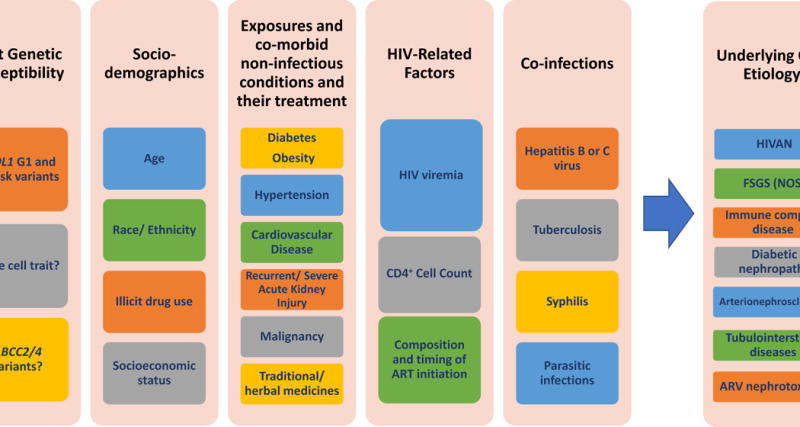
HIV-positive individuals are at increased risk for kidney disease, including HIV-associated nephropathy, noncollapsing focal segmental glomerulosclerosis, immune-complex kidney disease, and comorbid kidney disease, as well as kidney injury resulting from prolonged exposure to antiretroviral therapy or from opportunistic infections. Clinical guidelines for kidney disease prevention and treatment in HIV-positive individuals are largely extrapolated from studies in the general population, and do not fully incorporate existing knowledge of the unique HIV-related pathways and genetic factors that contribute to the risk of kidney disease in this population. We convened an international panel of experts in nephrology, renal pathology, and infectious diseases to define the pathology of kidney disease in the setting of HIV infection; describe the role of genetics in the natural history, diagnosis, and treatment of kidney disease in HIV-positive individuals; characterize the renal risk-benefit of antiretroviral therapy for HIV treatment and prevention; and define best practices for the prevention and management of kidney disease in HIV-positive individuals.
Keywords: APOL1; CKD progression; HIV; antiretroviral therapy; immune complex kidney disease; podocytopathy; renal pathology.
Copyright © 2017 International Society of Nephrology. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- UNAIDS. AIDSinfo. http://aidsinfo.unaids.org/ Accessed July 19, 2017)
-
- Rosenberg AZ, Naicker S, Winkler CA, et al. HIV-associated nephropathies: epidemiology, pathology, mechanisms and treatment. Nat Rev Nephrol. 2015;11:150–160. - PubMed
-
- D’Agati V, Appel GB. HIV infection and the kidney. J Am Soc Nephrol. 1997;8:138–152. - PubMed
-
- Ross MJ. Advances in the pathogenesis of HIV-associated kidney diseases. Kidney Int. 2014;86:266–274. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
