

Relationships Between Clinical Processes and Arteriovenous Fistula Cannulation and Maturation: A Multicenter Prospective Cohort Study
- PMID: 29398178
- PMCID: PMC5916528
- DOI: 10.1053/j.ajkd.2017.10.027
Relationships Between Clinical Processes and Arteriovenous Fistula Cannulation and Maturation: A Multicenter Prospective Cohort Study
Abstract
Background: Half of surgically created arteriovenous fistulas (AVFs) require additional intervention to effectively support hemodialysis. Postoperative care and complications may affect clinical maturation.
Study design: Hemodialysis Fistula Maturation (HFM) Study, a 7-center prospective cohort study.
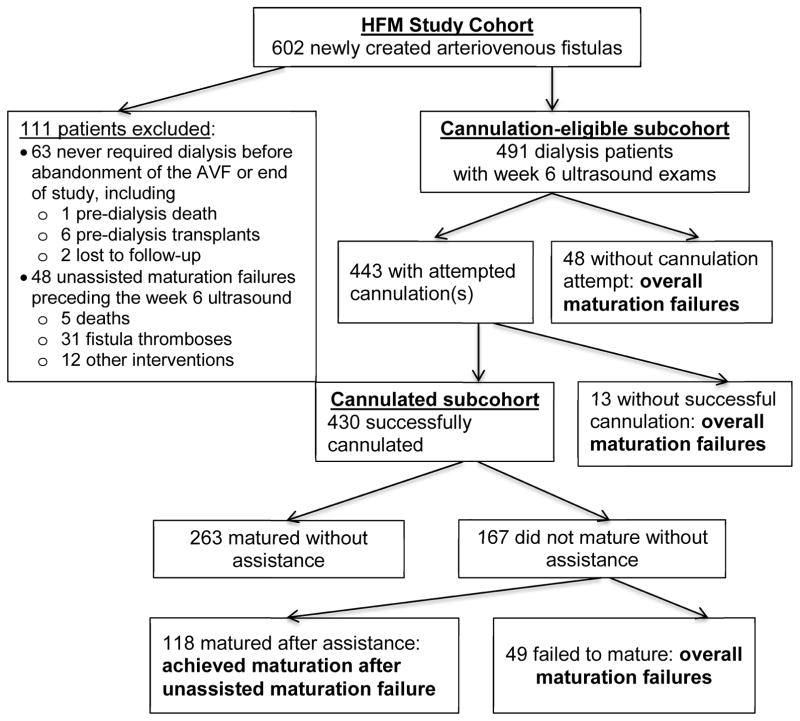
Setting & participants: 491 patients with single-stage AVFs who had neither thrombosis nor AVF intervention before a 6-week postoperative ultrasonographic examination and who required maintenance hemodialysis.
Predictors: Postoperative care processes and complications.
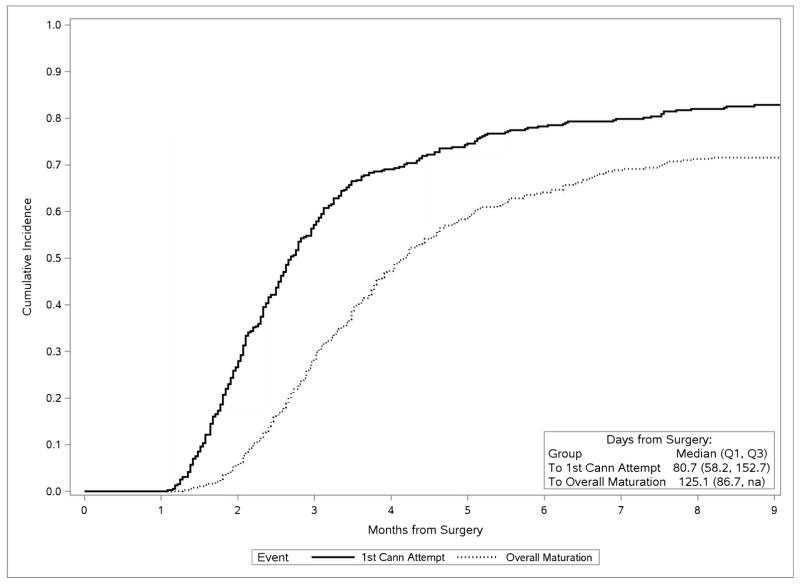
Outcomes: Attempted cannulation, successful cannulation, and unassisted and overall clinical maturation as defined by the HFM Study criteria.
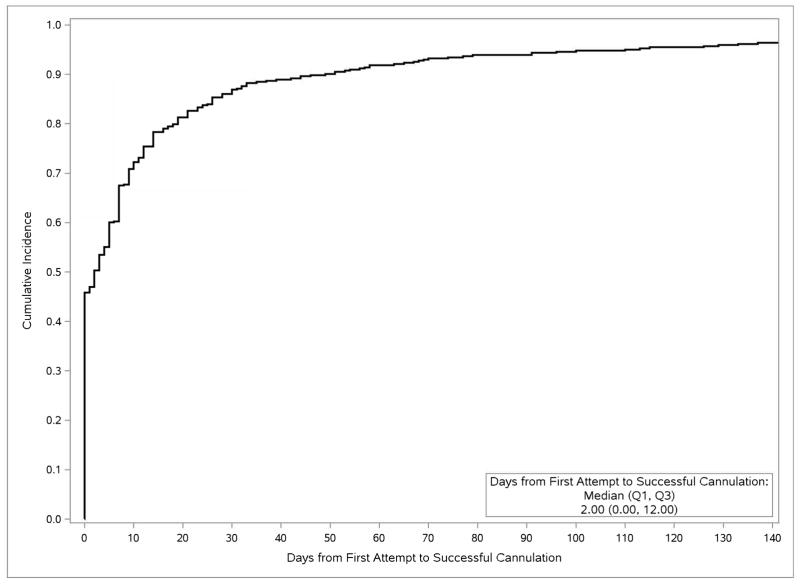
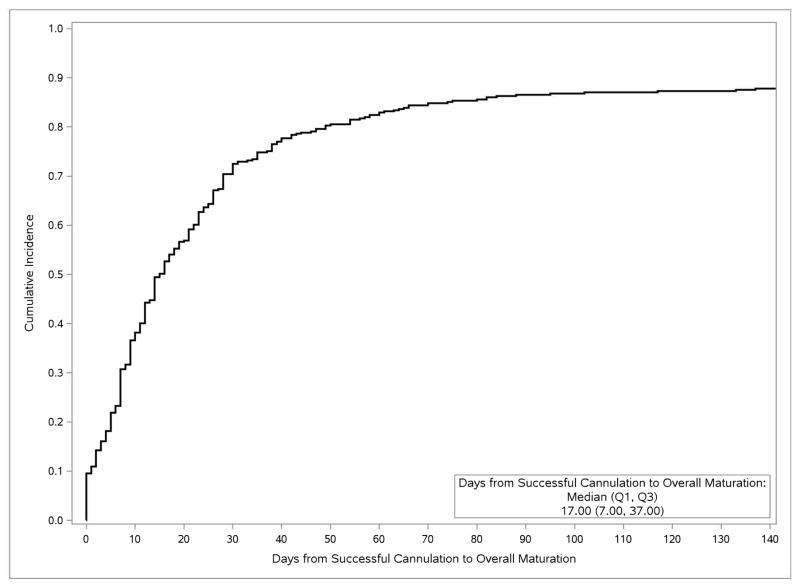
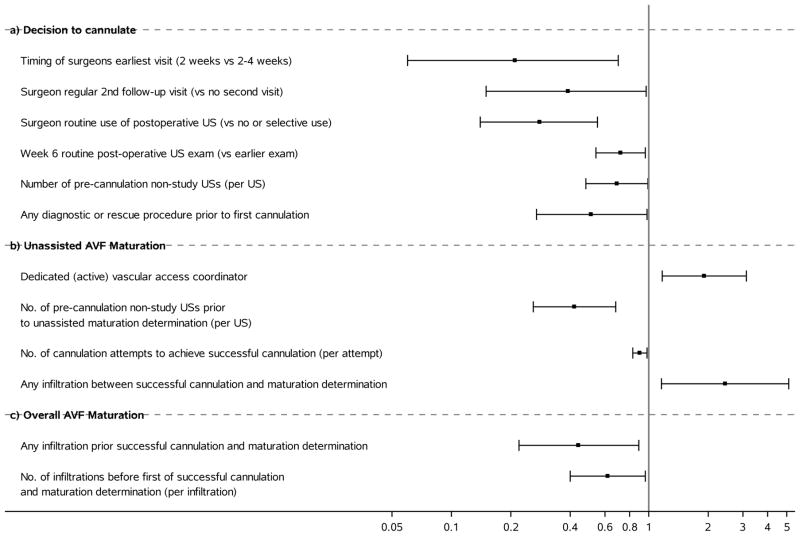
Results: AVF cannulation was attempted in 443 of 491 (90.2%) participants and was eventually successful in 430 of these 443 (97.1%) participants. 263 of these 430 (61.2%) reached unassisted and 118 (27.4%) reached assisted AVF maturation (overall maturation, 381/430 [88.6%]). Attempted cannulation was less likely in patients of surgeons with policies for routine 2-week versus later-than-2-week first postoperative visits (OR, 0.21; 95% CI, 0.06-0.70), routine second postoperative follow-up visits (OR, 0.39; 95% CI, 0.15-0.97), and a routine clinical postoperative ultrasound (OR, 0.28; 95% CI, 0.14-0.55). Attempted cannulation was also less likely among patients undergoing procedures to assist maturation (OR, 0.51; 95% CI, 0.27-0.98). Unassisted maturation was more likely for patients treated in facilities with access coordinators (OR, 1.91; 95% CI, 1.17-3.12), but less likely after precannulation nonstudy ultrasounds (OR per ultrasound, 0.42 [95% CI, 0.26-0.68]) and initial unsuccessful cannulation attempts (OR per each additional attempt, 0.90 [95% CI, 0.83-0.98]). Overall maturation was less likely with infiltration before successful cannulation (OR, 0.44; 95% CI, 0.22-0.89). Among participants receiving maintenance hemodialysis before AVF surgery, unassisted and overall maturation were less likely with longer intervals from surgery to initial cannulation (ORs for each additional month of 0.81 [95% CI, 0.76-0.88] and 0.93 [95% CI, 0.89-0.98], respectively) and from initial to successful cannulation (ORs for each additional week of 0.87 [95% CI, 0.81-0.94] and 0.88 [95% CI, 0.83-0.94], respectively).
Limitations: Surgeons' management policies were assessed only by questionnaire at study onset. Most participants received upper-arm AVFs, planned 2-stage AVFs were excluded, and maturation time windows were imposed. Some care processes may have been missed and the observational design limits causal attribution.
Conclusions: Multiple processes of care and complications are associated with AVF maturation outcomes.
Keywords: Vascular access; arteriovenous access; arteriovenous fistula (AVF); cannulation; end-stage renal disease; fistula maturation; hemodialysis; patency; process-of-care.
Copyright © 2017 National Kidney Foundation, Inc. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Asif A, Cherla G, Merrill D, Cipleu CD, Briones P, Pennell P. Conversion of tunneled hemodialysis catheter-consigned patients to arteriovenous fistula. Kidney Int. 2005;67(6):2399–2406. - PubMed
-
- McLafferty R, Pryor R, Johnson C, Ramsey D, Hodgson K. Outcome of a comprehensive follow-up program to enhance maturation of autogenous arteriovenous hemodialysis access. J Vasc Surg. 2007;45(5):981–985. - PubMed
-
- Flu H, Breslau P, Krol-van Straaten J, Hamming J, JWL The effect of implementation of an optimized care protocol on the outcome of arteriovenous hemodialysis access surgery. J Vasc Surg. 2008;48(3):659–668. - PubMed
-
- Kiaii M, MacRae J. A dedicated vascular access program can improve arteriovenous fistula rates without increasing catheters. J Vasc Access. 2008;9(4):254–259. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
