

Pregabalin Did Not Improve Pain Management After Spinal Fusions
- PMID: 29398993
- PMCID: PMC5786595
- DOI: 10.1007/s11420-017-9584-2
Pregabalin Did Not Improve Pain Management After Spinal Fusions
Abstract
Background: The treatment of postoperative pain is a challenge after posterior spinal fusions. Pain management using predominantly opioids is often associated with multiple adverse effects, while multimodal postoperative analgesia may provide adequate pain relief with fewer opioid side effects.
Questions/purposes: The purpose of this review is to determine whether addition of 150 mg pregabalin daily would reduce narcotic requirements and improve outcomes after posterior lumbar fusion (PLF).
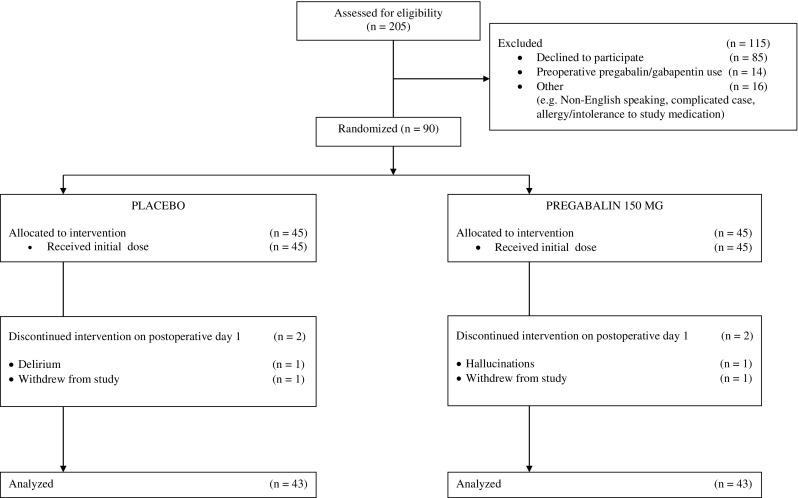
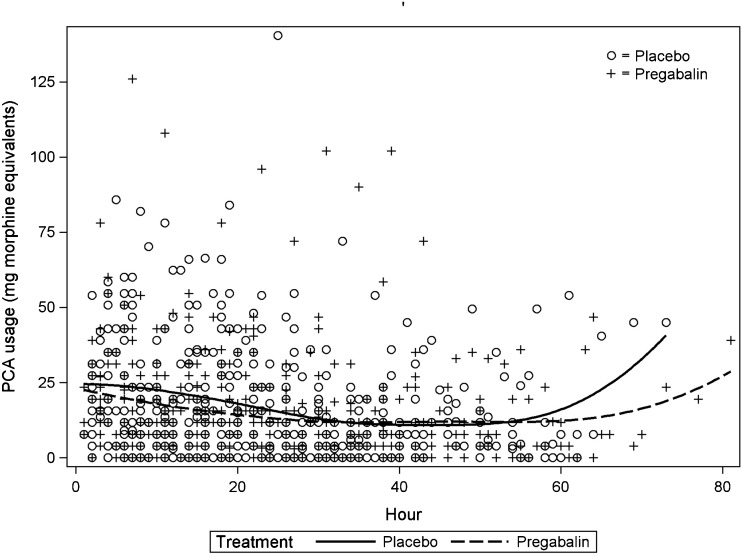
Methods: The method used is a randomized, controlled trial of elective PLF patients who received pregabalin or placebo. With institutional review board (IRB) approval, 86 patients undergoing elective posterior lumbar fusion, ASA I-III, were randomized to receive either a placebo or pregabalin after obtaining written informed consent. Both arms, i.e., placebo and pregabalin, consisted of 43 patients each.The 86 patients for elective PLF were randomly assigned to receive 150 mg of pregabalin 1 h before surgery and then 150 mg daily, or a placebo tablet. All patients received a similar general anesthetic and in the post-anesthesia care unit (PACU), started on intravenous (IV) patient-controlled analgesia (PCA) of hydromorphone (0.2 mg/ml). Postoperative pain was assessed daily until discharge using a Numerical Rating Scale (NRS) at rest and with physical therapy (PT). Patients were also assessed twice daily for level of sedation and nausea and/or vomiting and expected PT milestones. All narcotics (IV, oral) were documented.
Results: Demographics and operative time between groups were similar. PCA hydromorphone administration and oral narcotic intake were not statistically different between the two groups. However, an increased incidence of nausea and vomiting in the placebo group reached statistical significance (p < 0.05). In addition, there was no statistical difference between groups with respect to achieving PT milestones and hospital discharge day.
Conclusion: After PLF, patients receiving pregabalin 150 mg/day did not have reduced IV narcotic usage, improved PT milestones, or reduced length of hospital stay. We were unable to demonstrate an analgesic advantage to prescribing pregabalin to patients undergoing lumbar spinal fusions.
Keywords: multimodal analgesia; pain scores after spinal fusions; posterior lumbar fusions; postoperative analgesia; pregabalin.
Conflict of interest statement
Compliance with Ethical StandardsMichael K. Urban, MD, PhD; Kristy M. Labib, MD; Shane C. Reid, MBS, BA; Amanda K. Goon, BA; and Valeria Rotundo have declared that they have no conflict of interest. Frank P. Cammisa Jr MD reports royalties for patent with NuVasive. Federico P. Girardi, MD reports royalties paid for patents with DePuy Spine, LANX, Inc., NuVasive, and Ortho Development Corp., outside the work.All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2008 (5).Informed consent was obtained from all patients for being included in the study.Disclosure forms provided by the authors are available with the online version of this article.
Figures
References
-
- Buvanendran A, Kroin JS, Della Valle CJ, Kari M, Moric M, Tuman KJ. Perioperative oral pregabalin reduces chronic pain after total knee arthroplasty: a prospective, randomized, controlled trial. Anesth Analg. 2010; 110:199–207. 10.1213/ANE.0b013e3181c4273a. - PubMed
-
- Fletcher D, Martinez V. Opioid-induced hyperalgesia in patients after surgery: a systematic review and a meta-analysis. Br J Anaesth. 2014; 112:991–1004. 10.1093/bja/aeu137. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
