

Current state of follow-up care for patients with Hymenoptera venom anaphylaxis in southwest Germany: Major impact of early information
- PMID: 29399436
- PMCID: PMC5785614
- DOI: 10.1007/s40629-017-0046-7
Current state of follow-up care for patients with Hymenoptera venom anaphylaxis in southwest Germany: Major impact of early information
Abstract
Background: Up to 3.5% of the population experience anaphylactic reactions in response to Hymenoptera stings. Current guidelines are in place for the diagnostic workup and follow-up care of patients with Hymenoptera venom anaphylaxis (HVA). However, little is known about the degree of implementation of the recommendations and patient attitudes toward the recommendations in the general patient population.
Methods: For the analysis of the follow-up care in real life, a retrospective questionnaire-based study was conducted in unselected patients who had received treatment from an emergency medical response team for HVA, as documented in records of three regional Medical Emergency Response Centers.
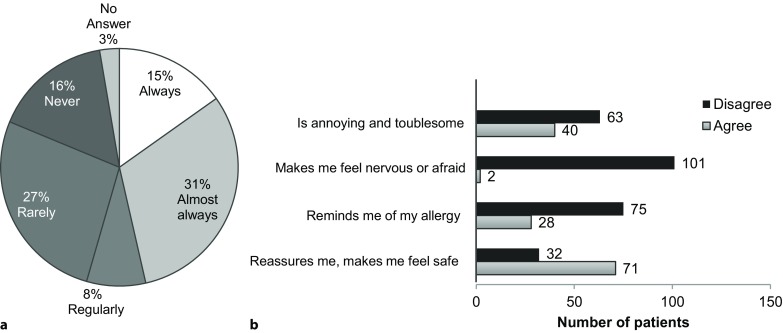
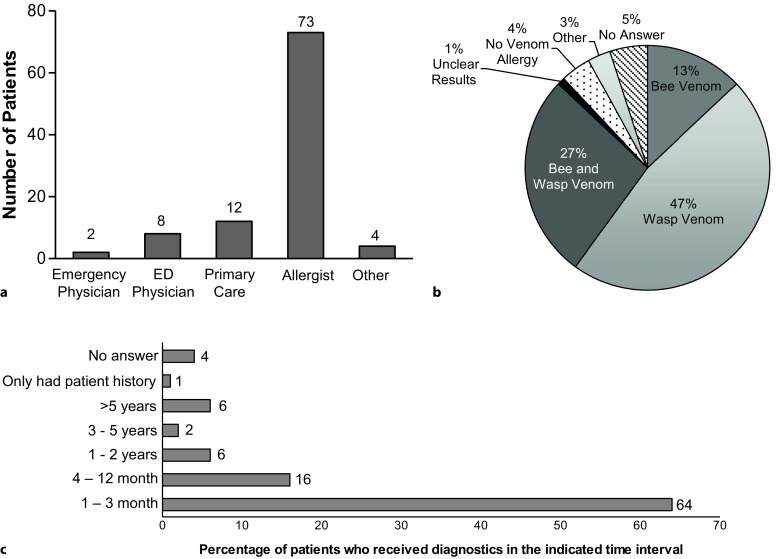
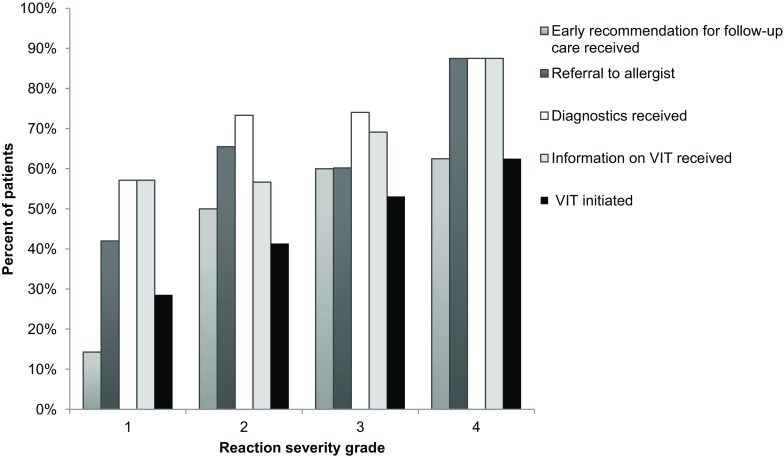
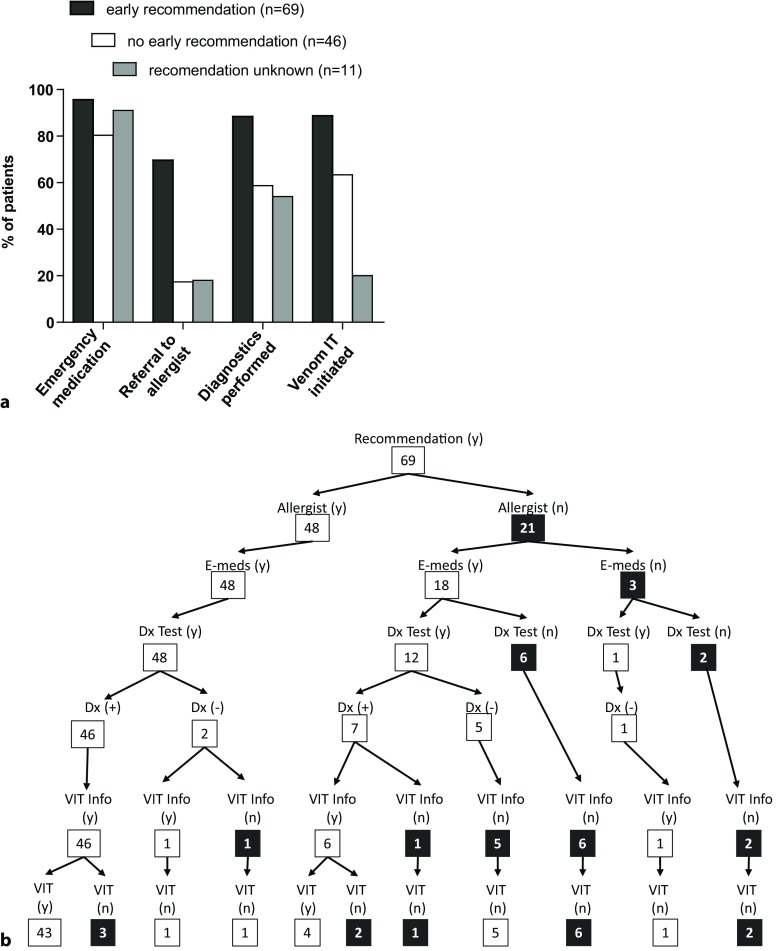
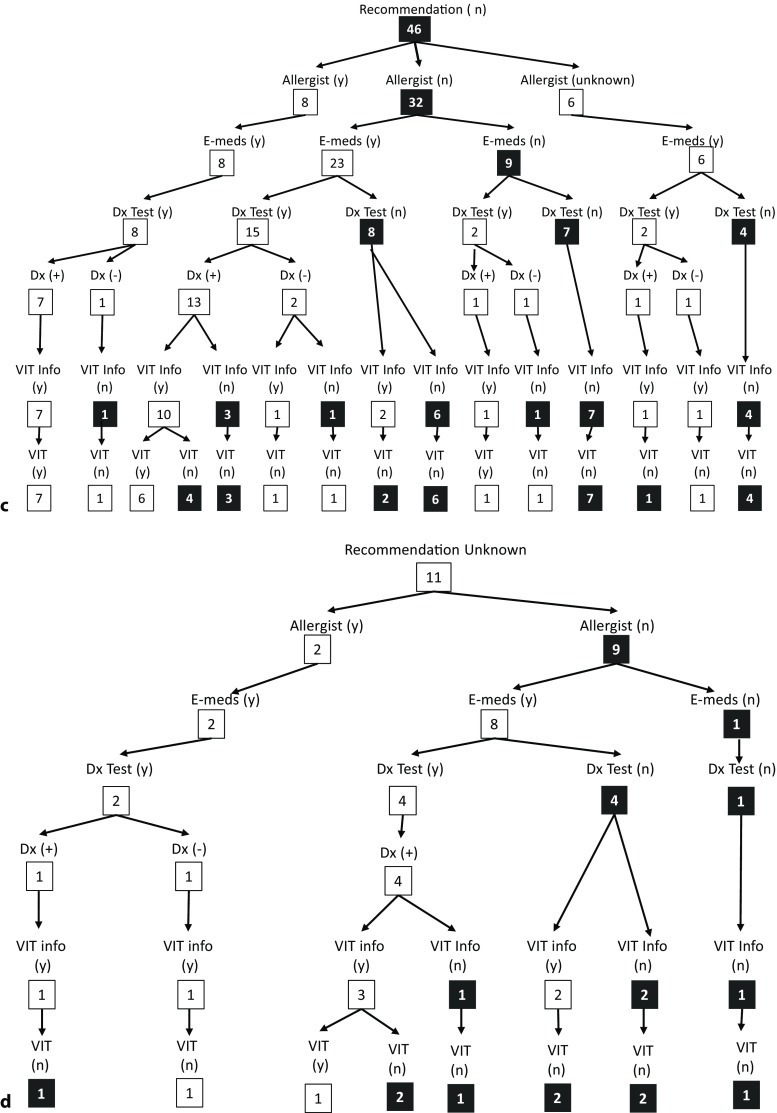
Results: From over 125,000 cases, a filtered list of 1895 patients that coded for anaphylaxis was generated and examination of paper records identified 548 patients with a documented insect sting anaphylaxis. Patients were sent a standardized questionnaire addressing different aspects of diagnostics and follow-up care. Almost 40% of the patients did not receive a referral to an allergist at the emergency center, over 50% did not consult an allergy specialist at any time after the index sting, 25% did not receive any form of diagnostic workup, over 30% did not receive any information about venom immunotherapy (VIT) as treatment option, and only 50% were eventually started on VIT. Emergency medication was prescribed in 90% of the cases, 77% including an adrenalin auto injector, of which 47% were expired at the time of the survey. Patients who were informed about diagnostic and treatment options early during the index event, i. e., during the stay in the emergency department, displayed a higher rate of referral to an allergist (70% vs. 17%), higher rate of diagnostic workup (88% vs. 59%), and a higher rate of initiation of VIT (89% vs. 64%), as compared to patients who did not.
Conclusion: Our results demonstrate that there are missed opportunities for secondary and tertiary prevention of anaphylaxis due to insect venom allergy and that early information on required diagnostics and treatment options has a major impact on the degree of proper follow-up care in line with current guideline recommendations.
Keywords: Anaphylaxis; Follow-up care; Guideline; Insect venom allergy.
Conflict of interest statement
T. Jakob has received research support from ALK-Abello, Allergy Therapeutics, Allergopharma, Cosmetics Europe, Novartis; speakers honoraria and consulting fees from ALK, Allergy Therapeutics, Allergopharma, Leti, and Novartis. M. Manmohan, S. Müller, M. Myriam Rauber, F. Koberne, H. Reisch, J. Koster, R. Böhm, M. Messelken and M. Fischer declare that they have no competing interests.
Figures
References
-
- Worm M, Dolle S, Francuzik W. Data from the anaphylaxis registry of the German-speaking countries. Rev Francaise D Allergol. 2015;55:452–455. doi: 10.1016/j.reval.2015.09.007. - DOI
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
