

Cost-effectiveness of WHO-Recommended Algorithms for TB Case Finding at Ethiopian HIV Clinics
- PMID: 29399596
- PMCID: PMC5788063
- DOI: 10.1093/ofid/ofx269
Cost-effectiveness of WHO-Recommended Algorithms for TB Case Finding at Ethiopian HIV Clinics
Abstract
Background: The World Health Organization (WHO) recommends active tuberculosis (TB) case finding and a rapid molecular diagnostic test (Xpert MTB/RIF) to detect TB among people living with HIV (PLHIV) in high-burden settings. Information on the cost-effectiveness of these recommended strategies is crucial for their implementation.
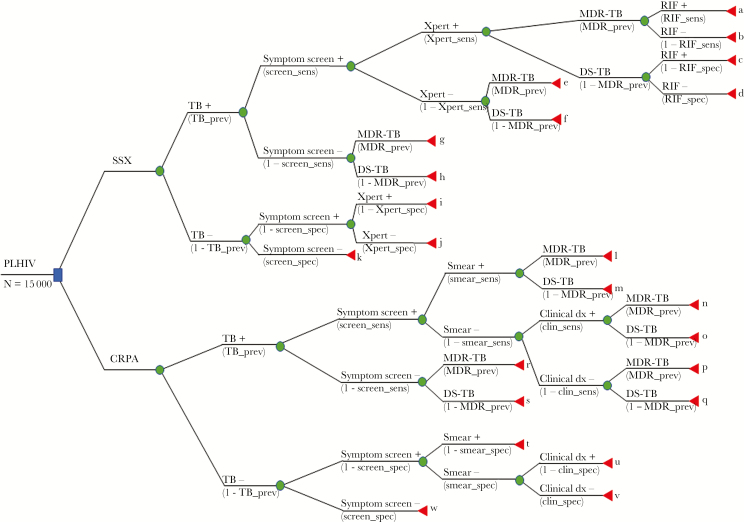
Methods: We conducted a model-based cost-effectiveness analysis comparing 2 algorithms for TB screening and diagnosis at Ethiopian HIV clinics: (1) WHO-recommended symptom screen combined with Xpert for PLHIV with a positive symptom screen and (2) current recommended practice algorithm (CRPA; based on symptom screening, smear microscopy, and clinical TB diagnosis). Our primary outcome was US$ per disability-adjusted life-year (DALY) averted. Secondary outcomes were additional true-positive diagnoses, and false-negative and false-positive diagnoses averted.
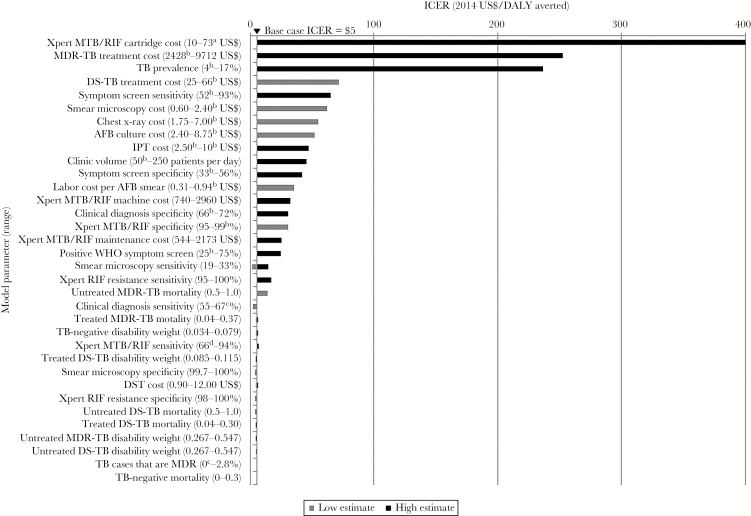
Results: Compared with CRPA, combining a WHO-recommended symptom screen with Xpert was highly cost-effective (incremental cost of $5 per DALY averted). Among a cohort of 15 000 PLHIV with a TB prevalence of 6% (900 TB cases), this algorithm detected 8 more true-positive cases than CRPA, and averted 2045 false-positive and 8 false-negative diagnoses compared with CRPA. The WHO-recommended algorithm was marginally costlier ($240 000) than CRPA ($239 000). In sensitivity analysis, the symptom screen/Xpert algorithm was dominated at low Xpert sensitivity (66%).
Conclusions: In this model-based analysis, combining a WHO-recommended symptom screen with Xpert for TB diagnosis among PLHIV was highly cost-effective ($5 per DALY averted) and more sensitive than CRPA in a high-burden, resource-limited setting.
Keywords: Ethiopia; TB/HIV co-infection; cost-effectiveness; developing countries; modeling.
Figures
References
-
- World Health Organization. Guidelines for intensified tuberculosis case-finding and isoniazid preventive therapy for people living with HIV in resource-constrained settings 2011. Available at: http://whqlibdoc.who.int/publications/2011/9789241500708_eng.pdf. Accessed 20 August 2014.
-
- World Health Organization. Global tuberculosis report 2016 2016. Available at: http://apps.who.int/iris/bitstream/10665/250441/1/9789241565394-eng.pdf?.... Accessed 2 February 2017.
-
- World Health Organization. Tuberculosis financing and funding gaps Available at: http://www.who.int/tb/WHO_GF_TB_financing_factsheet.pdf. Published 2013. Accessed 20 August 2014.
-
- Mann G, Squire SB, Bissell K et al. Beyond accuracy: creating a comprehensive evidence base for TB diagnostic tools. Int J Tuberc Lung Dis 2010; 14:1518–24. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
