

Systematic review and meta-analysis of cannabinoids in palliative medicine
- PMID: 29400010
- PMCID: PMC5879974
- DOI: 10.1002/jcsm.12273
Systematic review and meta-analysis of cannabinoids in palliative medicine
Abstract
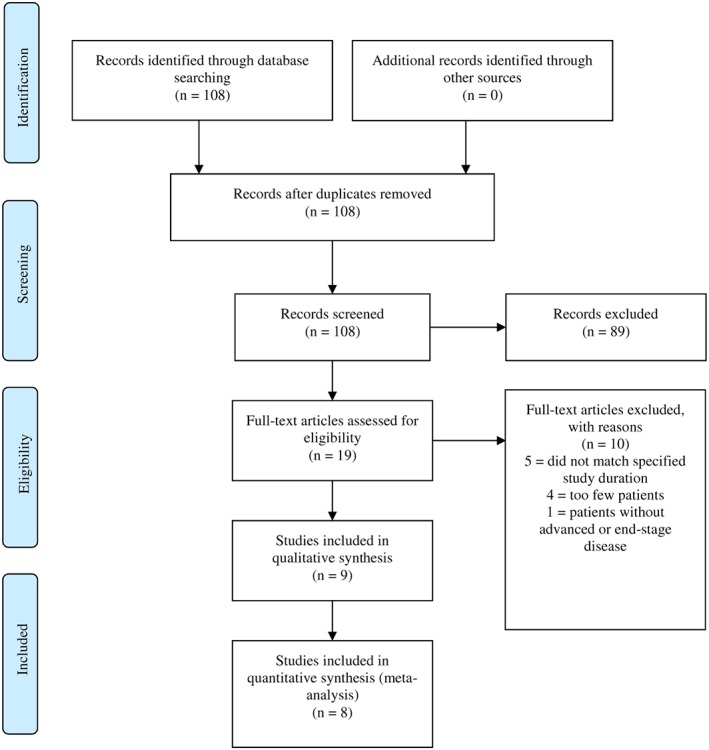
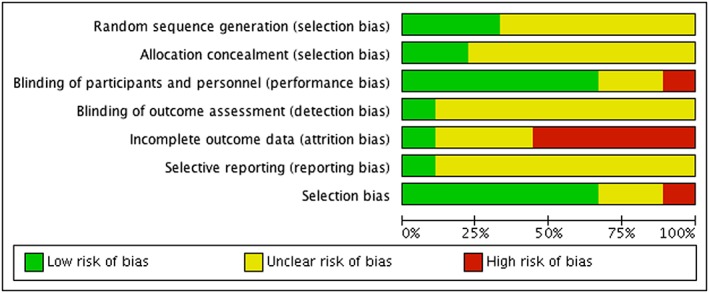
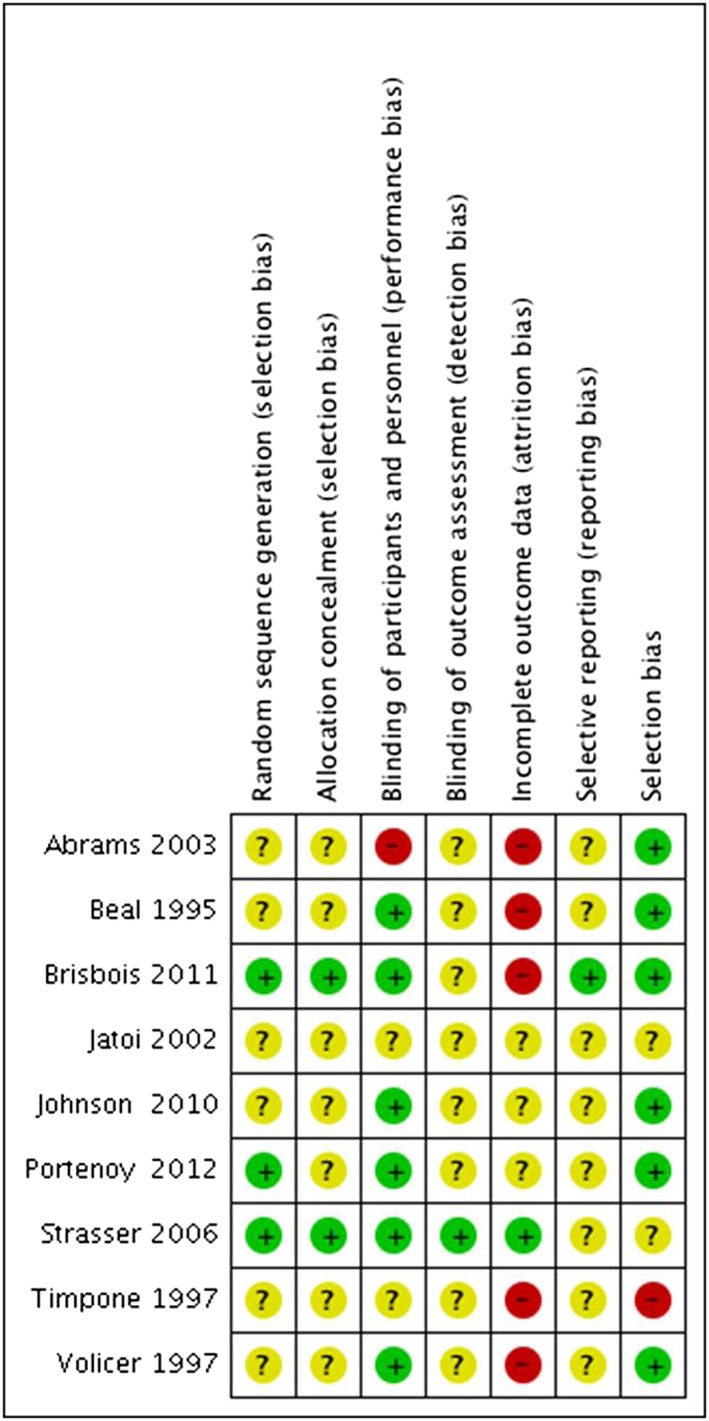
We provide a systematic review and meta-analysis on the efficacy, tolerability, and safety of cannabinoids in palliative medicine. The Cochrane Central Register of Controlled Trials (CENTRAL), MEDLINE, PsycINFO, PubMed, Scopus, and http://clinicaltrials.gov, and a selection of cancer journals were searched up until 15th of March 2017. Of the 108 screened studies, nine studies with a total of 1561 participants were included. Overall, the nine studies were at moderate risk of bias. The quality of evidence comparing cannabinoids with placebo was rated according to Grading of Recommendations Assessment, Development, and Evaluation as low or very low because of indirectness, imprecision, and potential reporting bias. In cancer patients, there were no significant differences between cannabinoids and placebo for improving caloric intake (standardized mean differences [SMD]: 0.2 95% confidence interval [CI]: [-0.66, 1.06] P = 0.65), appetite (SMD: 0.81 95% CI: [-1.14, 2.75]; P = 0.42), nausea/vomiting (SMD: 0.21 [-0.10, 0.52] P = 0.19), >30% decrease in pain (risk differences [RD]: 0.07 95% CI: [-0.01, 0.16]; P = 0.07), or sleep problems (SMD: -0.09 95% CI: [-0.62, 0.43] P = 0.72). In human immunodeficiency virus (HIV) patients, cannabinoids were superior to placebo for weight gain (SMD: 0.57 [0.22; 0.92]; P = 0.001) and appetite (SMD: 0.57 [0.11; 1.03]; P = 0.02) but not for nausea/vomiting (SMD: 0.20 [-0.15, 0.54]; P = 0.26). Regarding side effects in cancer patients, there were no differences between cannabinoids and placebo in symptoms of dizziness (RD: 0.03 [-0.02; 0.08]; P = 0.23) or poor mental health (RD: -0.01 [-0.04; 0.03]; P = 0.69), whereas in HIV patients, there was a significant increase in mental health symptoms (RD: 0.05 [0.00; 0.11]; P = 0.05). Tolerability (measured by the number of withdrawals because of adverse events) did not differ significantly in cancer (RD: 1.15 [0.80; 1.66]; P = 0.46) and HIV patients (RD: 1.87 [0.60; 5.84]; P = 0.28). Safety did not differ in cancer (RD: 1.12 [0.86; 1.46]; P = 0.39) or HIV patients (4.51 [0.54; 37.45]; P = 0.32) although there was large uncertainty about the latter reflected in the width of the CI. In one moderate quality study of 469 cancer patients with cancer-associated anorexia, megestrol was superior to cannabinoids in improving appetite, producing >10% weight gain and tolerability. In another study comparing megestrol to dronabinol in HIV patients, megestrol treatment led to higher weight gain without any differences in tolerability and safety. We found no convincing, unbiased, high quality evidence suggesting that cannabinoids are of value for anorexia or cachexia in cancer or HIV patients.
Keywords: HIV; cancer; cannabinoids; marijuana; palliation; systematic review; weight gain.
© 2018 The Authors. Journal of Cachexia, Sarcopenia and Muscle published by John Wiley & Sons Ltd on behalf of the Society on Sarcopenia, Cachexia and Wasting Disorders.
Figures
References
-
- World Health Organisation . Palliative Care Fact Sheet No. 402 2015 [cited 2017. February 8]; Available from: http://www.who.int/mediacentre/factsheets/fs402/en/.
-
- Van Mechelen W, Aertgeerts B, De Ceulaer K, Thoonsen B, Vermandere M, Warmenhoven F, et al. Defining the palliative care patient: a systematic review. Palliat Med 2013;27:197–208. - PubMed
-
- Sigurdardottir KR, Kaasa S, Rosland JH, Bausewein C, Radbruch L, Haugen DF, et al. The European Association for palliative care basic dataset to describe a palliative care cancer population: results from an international Delphi process. Palliat Med 2014;28:463–473. - PubMed
-
- Van Lancker A, Velghe A, Van Hecke A, Verbrugghe M, Van Den Noortgate N, Grypdonck M, et al. Prevalence of symptoms in older cancer patients receiving palliative care: a systematic review and meta‐analysis. J Pain Symptom Manage 2014;47:90–104. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
