

Phosphatidylinositol 3-Kinase α-Selective Inhibition With Alpelisib (BYL719) in PIK3CA-Altered Solid Tumors: Results From the First-in-Human Study
- PMID: 29401002
- PMCID: PMC5920739
- DOI: 10.1200/JCO.2017.72.7107
Phosphatidylinositol 3-Kinase α-Selective Inhibition With Alpelisib (BYL719) in PIK3CA-Altered Solid Tumors: Results From the First-in-Human Study
Erratum in
Abstract
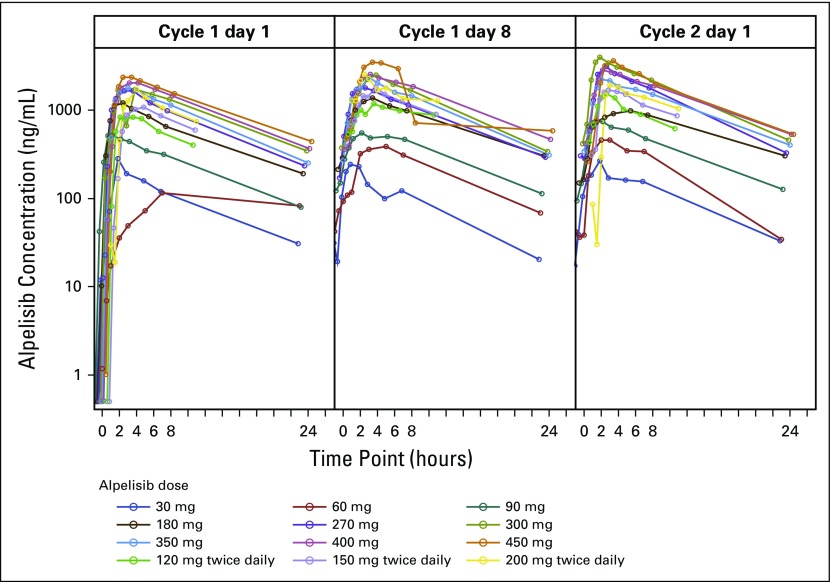
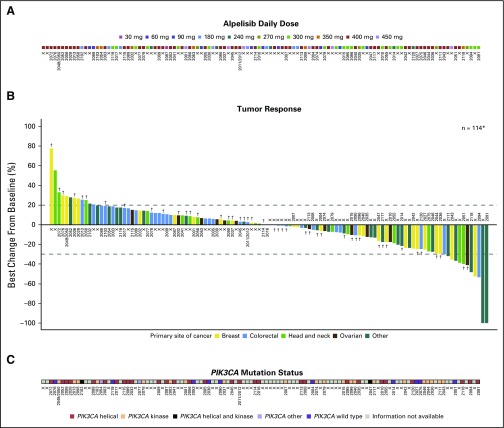
Purpose We report the first-in-human phase Ia study to our knowledge ( ClinicalTrials.gov identifier: NCT01219699) identifying the maximum tolerated dose and assessing safety and preliminary efficacy of single-agent alpelisib (BYL719), an oral phosphatidylinositol 3-kinase α (PI3Kα)-selective inhibitor. Patients and Methods In the dose-escalation phase, patients with PIK3CA-altered advanced solid tumors received once-daily or twice-daily oral alpelisib on a continuous schedule. In the dose-expansion phase, patients with PIK3CA-altered solid tumors and PIK3CA-wild-type, estrogen receptor-positive/human epidermal growth factor receptor 2-negative breast cancer received alpelisib 400 mg once daily. Results One hundred thirty-four patients received treatment. Alpelisib maximum tolerated doses were established as 400 mg once daily and 150 mg twice daily. Nine patients (13.2%) in the dose-escalation phase had dose-limiting toxicities of hyperglycemia (n = 6), nausea (n = 2), and both hyperglycemia and hypophosphatemia (n = 1). Frequent all-grade, treatment-related adverse events included hyperglycemia (51.5%), nausea (50.0%), decreased appetite (41.8%), diarrhea (40.3%), and vomiting (31.3%). Alpelisib was rapidly absorbed; half-life was 7.6 hours at 400 mg once daily with minimal accumulation. Objective tumor responses were observed at doses ≥ 270 mg once daily; overall response rate was 6.0% (n = 8; one patient with endometrial cancer had a complete response, and seven patients with cervical, breast, endometrial, colon, and rectal cancers had partial responses). Stable disease was achieved in 70 (52.2%) patients and was maintained > 24 weeks in 13 (9.7%) patients; disease control rate (complete and partial responses and stable disease) was 58.2%. In patients with estrogen receptor-positive/human epidermal growth factor receptor 2-negative breast cancer, median progression-free survival was 5.5 months. Frequently mutated genes (≥ 10% tumors) included TP53 (51.3%), APC (23.7%), KRAS (22.4%), ARID1A (13.2%), and FBXW7 (10.5%). Conclusion Alpelisib demonstrated a tolerable safety profile and encouraging preliminary activity in patients with PIK3CA-altered solid tumors, supporting the rationale for selective PI3Kα inhibition in combination with other agents for the treatment of PIK3CA-mutant tumors.
Figures
Comment in
-
The PI3Kα Inhibitor Alpelisib Has Activity in PIK3CA-altered Tumors.Cancer Discov. 2018 Apr;8(4):OF7. doi: 10.1158/2159-8290.CD-RW2018-027. Epub 2018 Feb 16. Cancer Discov. 2018. PMID: 29453241
-
Isoform-Selective Phosphatidylinositol 3-Kinase Inhibition in Cancer.J Clin Oncol. 2018 May 1;36(13):1339-1342. doi: 10.1200/JCO.2017.77.0891. Epub 2018 Mar 8. J Clin Oncol. 2018. PMID: 29517943 No abstract available.
References
-
- Shaw RJ, Cantley LC: Ras, PI(3)K and mTOR signalling controls tumour cell growth. Nature 441:424-430, 2006 - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
