

Prognostic Role of High-sensitivity Cardiac Troponin I and Soluble Suppression of Tumorigenicity-2 in Surgical Intensive Care Unit Patients Undergoing Non-cardiac Surgery
- PMID: 29401554
- PMCID: PMC5820064
- DOI: 10.3343/alm.2018.38.3.204
Prognostic Role of High-sensitivity Cardiac Troponin I and Soluble Suppression of Tumorigenicity-2 in Surgical Intensive Care Unit Patients Undergoing Non-cardiac Surgery
Abstract
Background: The prognostic utility of cardiac biomarkers, high-sensitivity cardiac troponin I (hs-cTnI) and soluble suppression of tumorigenicity-2 (sST2), in non-cardiac surgery is not well-defined. We evaluated hs-cTnI and sST2 as predictors of 30-day major adverse cardiac events (MACE) in patients admitted to the surgical intensive care unit (SICU) following major non-cardiac surgery.
Methods: hs-cTnI and sST2 concentrations were measured in 175 SICU patients immediately following surgery and for three days postoperatively. The results were analyzed in relation to 30-day MACE and were compared with the revised Goldman cardiac risk index (RCRI) score.
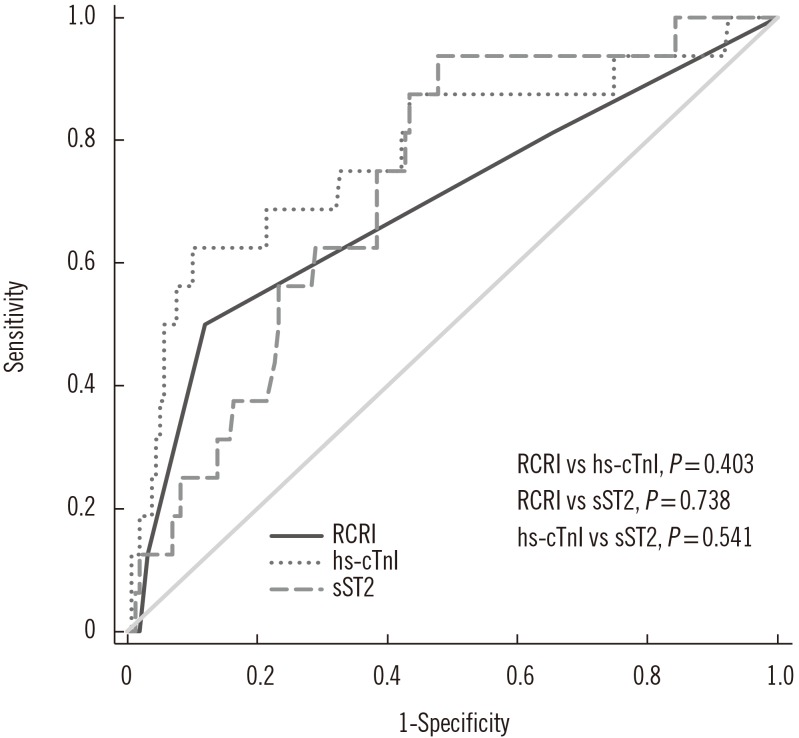
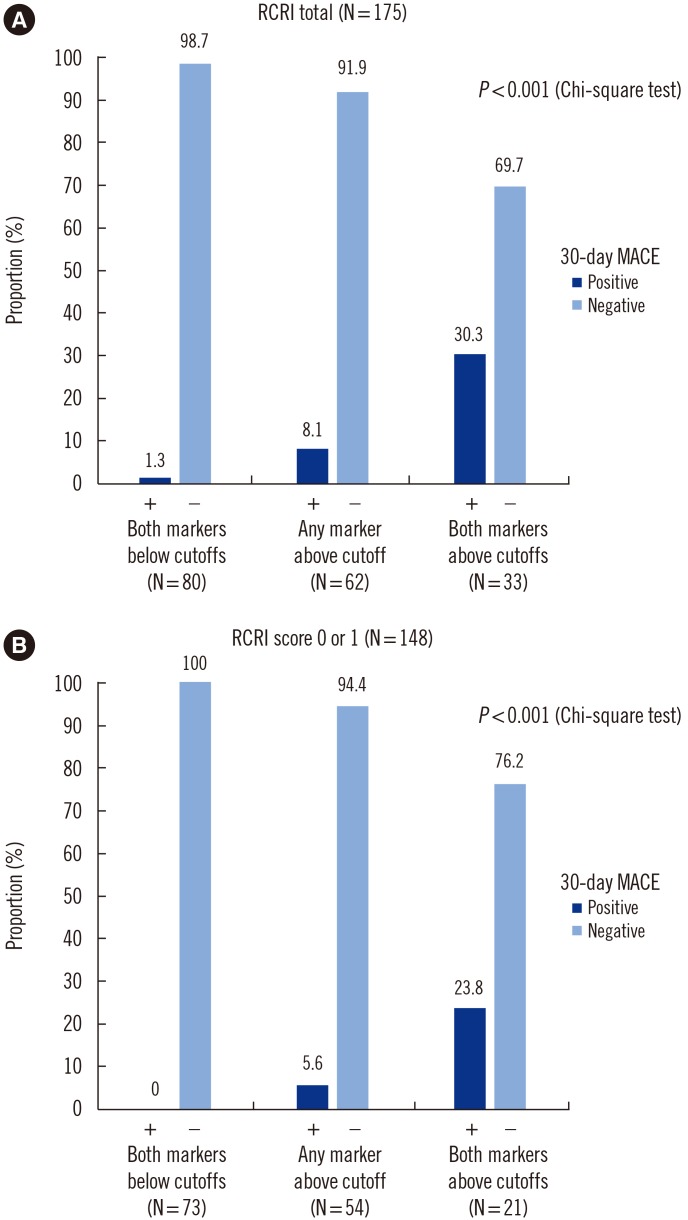
Results: Overall, 30-day MACE was observed in 16 (9.1%) patients. hs-cTnI and sST2 concentrations differed significantly between the two groups with and without 30-day MACE (P<0.05). The maximum concentration of sST2 was an independent predictor of 30-day MACE (odds ratio=1.016, P=0.008). The optimal cut-off values of hs-cTnI and sST2 for predicting 30-day MACE were 53.0 ng/L and 182.5 ng/mL, respectively. A combination of hs-cTnI and sST2 predicted 30-day MACE better than the RCRI score. Moreover, 30-day MACE was observed more frequently with increasing numbers of above-optimal cut-off hs-cTnI and sST2 values (P<0.0001). Reclassification analyses indicated that the addition of biomarkers to RCRI scores improved the prediction of 30-day MACE.
Conclusions: This study demonstrates the utility of hs-cTnI and sST2 in predicting 30-day MACE following non-cardiac surgery. Cardiac biomarkers would provide enhanced risk stratification in addition to clinical RCRI scores for patients undergoing major non-cardiac surgery.
Keywords: High-sensitivity cardiac troponin I; Non-cardiac surgery; Prognosis; Soluble suppression of tumorigenicity-2.
© The Korean Society for Laboratory Medicine
Conflict of interest statement
No potential conflicts of interest relevant to this study are reported.
Figures
References
-
- McCarthy CP, van Kimmenade RRJ, Gaggin HK, Simon ML, Ibrahim NE, Gandhi P, et al. Usefulness of multiple biomarkers for predicting incident major adverse cardiac events in patients who underwent diagnostic coronary angiography (from the Catheter Sampled Blood Archive in Cardiovascular Disease [CASABLANCA] Study) Am J Cardiol. 2017;120:25–32. - PubMed
-
- Kip KE, Hollabaugh K, Marroquin OC, Williams DO. The problem with composite end points in cardiovsacular studies. J Am Coll Cardiol. 2008;51:701–707. - PubMed
-
- Khuri SF, Daley J, Henderson W, Hur K, Demakis J, Aust JB, et al. The Department of Veterans Affairs’ NSQIP: the first national, validated, outcome-based, risk-adjusted, and peer-controlled program for the measurement and enhancement of the quality of surgical care. National VA Surgical Quality Improvement Program. Ann Surg. 1998;228:491–507. - PMC - PubMed
-
- Lee TH, Marcantonio ER, Mangione CM, Thomas EJ, Polanczyk CA, Cook EF, et al. Derivation and prospective validation of a simple index for prediction of cardiac risk of major noncardiac surgery. Circulation. 1999;100:1043–1049. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
