

Economic evaluation of an extended nutritional intervention in older Australian hospitalized patients: a randomized controlled trial
- PMID: 29402228
- PMCID: PMC5799921
- DOI: 10.1186/s12877-018-0736-0
Economic evaluation of an extended nutritional intervention in older Australian hospitalized patients: a randomized controlled trial
Abstract
Background: Prevalence of malnutrition in older hospitalized patients is 30%. Malnutrition is associated with poor clinical outcomes in terms of high morbidity and mortality and is costly for hospitals. Extended nutrition interventions improve clinical outcomes but limited studies have investigated whether these interventions are cost-effective.
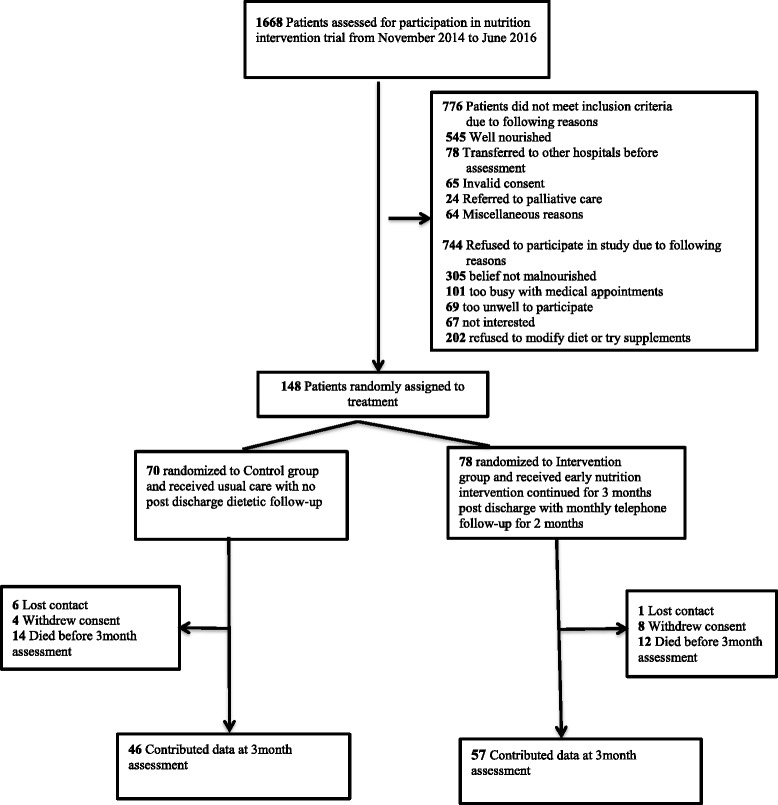
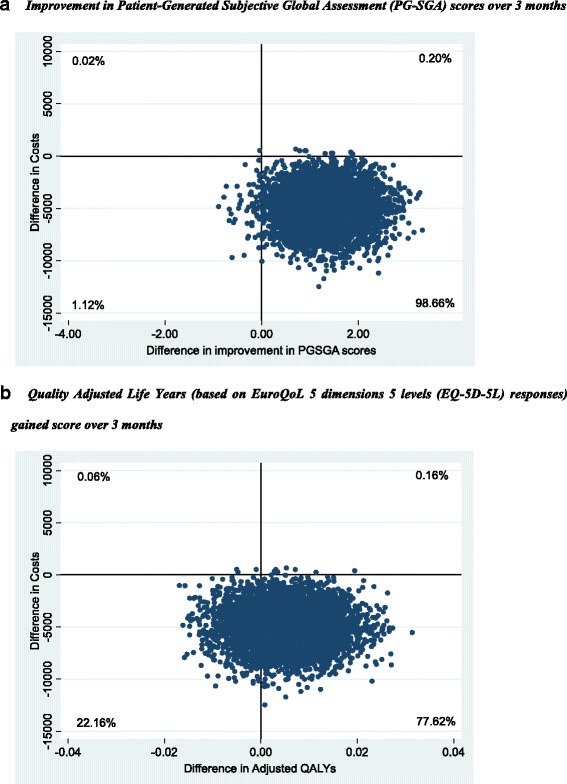
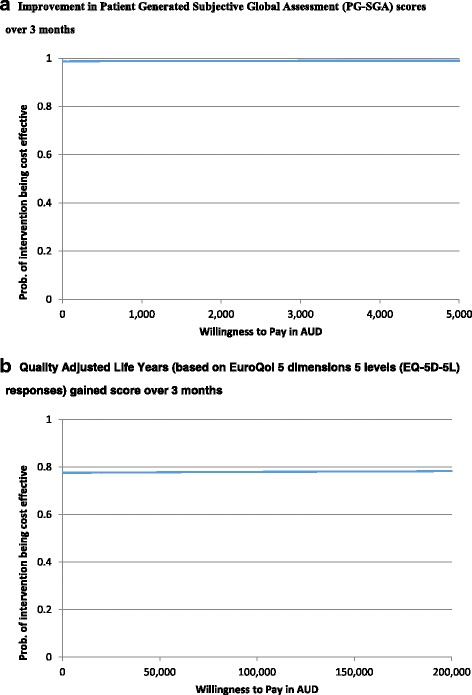
Methods: In this randomized controlled trial, 148 malnourished general medical patients ≥60 years were recruited and randomized to receive either an extended nutritional intervention or usual care. Nutrition intervention was individualized and started with 24 h of admission and was continued for 3 months post-discharge with a monthly telephone call whereas control patients received usual care. Nutrition status was confirmed by Patient generated subjective global assessment (PG-SGA) and health-related quality of life (HRQoL) was measured using EuroQoL 5D (EQ-5D-5 L) questionnaire at admission and at 3-months follow-up. A cost-effectiveness analysis was conducted for the primary outcome (incremental costs per unit improvement in PG-SGA) while a cost-utility analysis (CUA) was undertaken for the secondary outcome (incremental costs per quality adjusted life year (QALY) gained).
Results: Nutrition status and HRQoL improved in intervention patients. Mean per included patient Australian Medicare costs were lower in intervention group compared to control arm (by $907) but these differences were not statistically significant (95% CI: -$2956 to $4854). The main drivers of higher costs in the control group were higher inpatient ($13,882 versus $13,134) and drug ($838 versus $601) costs. After adjusting outcomes for baseline differences and repeated measures, the intervention was more effective than the control with patients in this arm reporting QALYs gained that were higher by 0.0050 QALYs gained per patient (95% CI: -0.0079 to 0.0199). The probability of the intervention being cost-effective at willingness to pay values as low as $1000 per unit improvement in PG-SGA was > 98% while it was 78% at a willingness to pay $50,000 per QALY gained.
Conclusion: This health economic analysis suggests that the use of extended nutritional intervention in older general medical patients is likely to be cost-effective in the Australian health care setting in terms of both primary and secondary outcomes.
Trial registration: ACTRN No. 12614000833662 . Registered 6 August 2014.
Keywords: Economic evaluation; Health related quality of life; Malnutrition; Older patients; Quality adjusted life years.
Conflict of interest statement
Ethics approval and consent to participate
This study was approved by Southern Adelaide Human Research Ethics (SA HREC) committee approval number 273.1. This trial was prospectively registered with Australia and New Zealand clinical trial registry No ACTRN12614000833662 on 6 August 2014. Written informed consent was taken from all the participants.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Sharma Y, Thompson C, Shahi R, Hakendorf P, Miller M. Malnutrition in acutely unwell hospitalized elderly - “The skeletons are still rattling in the hospital closet”. J Nutr 2017; doi:10.1007/s12603-017-0903-61-6. - PubMed
-
- Russell CA. The impact of malnutrition on healthcare costs and economic considerations for the use of oral nutritional supplements. Clin Nutr. 2007;2:25–32.
-
- Kruizenga HM, Van Tulder MW, Seidell JC, Thijs A, Ader HJ, Van Bokhorst-de van der Schueren MA. Effectiveness and cost-effectiveness of early screening and treatment of malnourished patients. Am J Clin Nutr. 2005;82:1082–1089. - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
