

Laparoscopic low anterior resection for rectal cancer with rectal prolapse: a case report
- PMID: 29402298
- PMCID: PMC5799977
- DOI: 10.1186/s13256-017-1555-1
Laparoscopic low anterior resection for rectal cancer with rectal prolapse: a case report
Abstract
Background: Rectal cancer with rectal prolapse is rare, described by only a few case reports. Recently, laparoscopic surgery has become standard procedure for either rectal cancer or rectal prolapse. However, the use of laparoscopic low anterior resection for rectal cancer with rectal prolapse has not been reported.
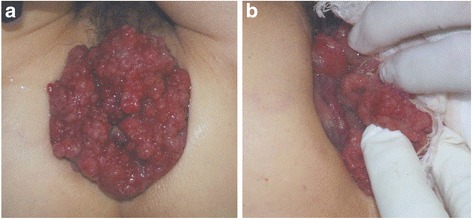
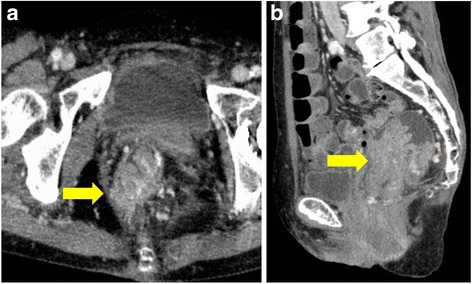
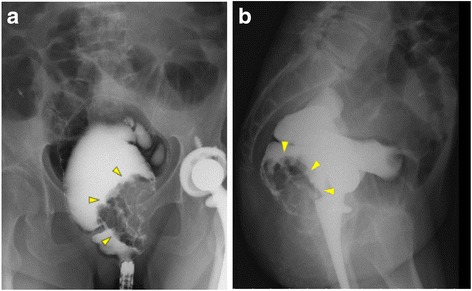
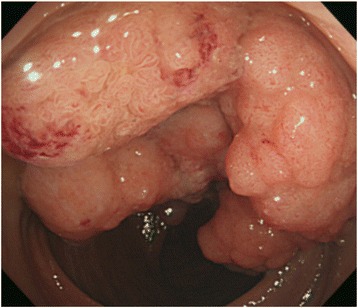
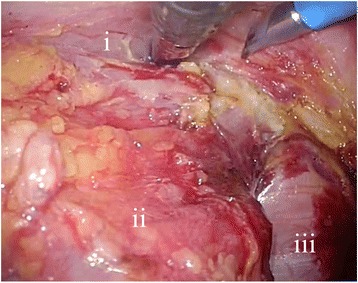
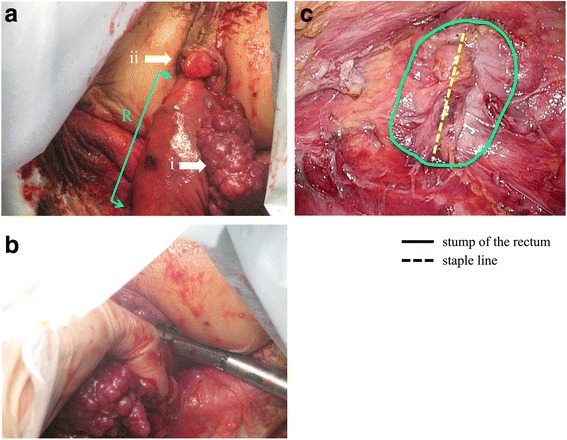
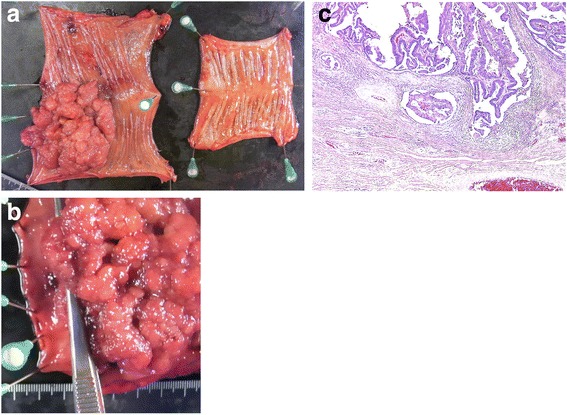
Case presentation: A 63-year-old Japanese woman suffered from rectal prolapse, with a mass and rectal bleeding for 2 years. An examination revealed complete rectal prolapse and the presence of a soft tumor, 7 cm in diameter; the distance from the anal verge to the tumor was 5 cm. Colonoscopy demonstrated a large villous tumor in the lower rectum, which was diagnosed as adenocarcinoma on biopsy. We performed laparoscopic low anterior resection using the prolapsing technique without rectopexy. The distal surgical margin was more than 1.5 cm from the tumor. There were no major perioperative complications. Twelve months after surgery, our patient is doing well with no evidence of recurrence of either the rectal prolapse or the cancer, and she has not suffered from either fecal incontinence or constipation.
Conclusions: Laparoscopic low anterior resection without rectopexy can be an appropriate surgical procedure for rectal cancer with rectal prolapse. The prolapsing technique is useful in selected patients.
Keywords: Laparoscopic; Low anterior resection; Prolapsing technique; Rectal cancer; Rectal prolapse.
Conflict of interest statement
Ethics approval and consent to participate
The institutional ethics committee approved the publication of this case report.
Consent for publication
Written informed consent was obtained from the patient for publication of this case report and any accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- van der Pas MH, Haglind E, Cuesta MA, Fürst A, Lacy AM, Hop WC, Colorectal cancer Laparoscopic or Open Resection II (COLOR II) Study Group et al. Laparoscopic versus open surgery for rectal cancer (COLOR II): short-term outcomes of a randomised, phase 3 trial. Lancet Oncol. 2013;14:210–8. doi: 10.1016/S1470-2045(13)70016-0. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
