

Morphologic Analysis of the Normal Right Ventricle Using Three-Dimensional Echocardiography-Derived Curvature Indices
- PMID: 29402505
- PMCID: PMC5936650
- DOI: 10.1016/j.echo.2017.12.009
Morphologic Analysis of the Normal Right Ventricle Using Three-Dimensional Echocardiography-Derived Curvature Indices
Abstract
Background: Right ventricular (RV) remodeling involves changes in size, wall thickness, function, and shape. Previous studies have suggested that regional curvature indices (rCI) may be useful for RV shape analysis. The aim of this study was to establish normal three-dimensional echocardiographic values of rCI in a large group of healthy subjects to facilitate future three-dimensional echocardiographic study of adverse RV remodeling.
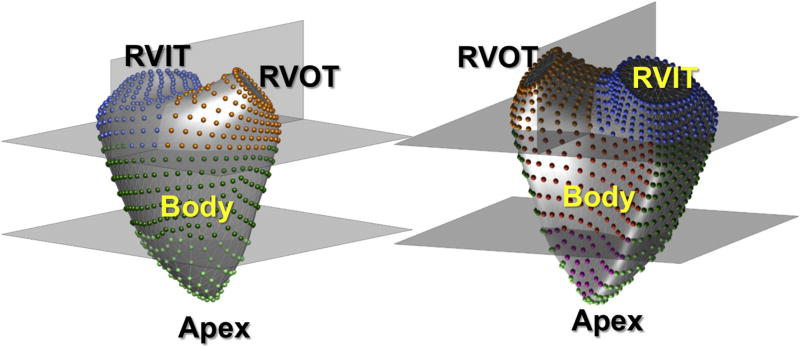
Methods: RV endocardial surfaces were reconstructed at end-diastole and end-systole in 245 healthy subjects (mean age, 42 ± 12 years) and analyzed using custom software to calculate mean curvature in six regions: RV inflow tract (RVIT) and RV outflow tract, apex, and body (both divided into free wall and septal regions). Associations with age and gender were studied.
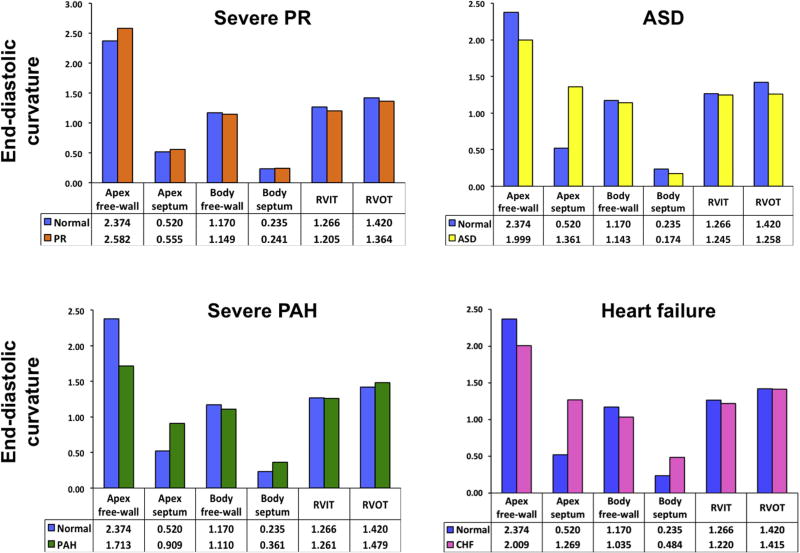
Results: The apical free wall was convex, while the septum (apex and body) was more concave than the body free wall. Septal curvature did not change significantly from end-diastole to end-systole. The RV outflow tract and RVIT became flatter from end-diastole to end-systole. In keeping with the "bellows-like" action of RV contraction, the body free wall became flatter, while the apex free wall changed to a more convex surface. There were no intergender differences in rCI. In older subjects (≥55 years of age), the RV free wall and RV outflow tract were flatter, and from end-diastole to end-systole, the RVIT became less flattened and the apex less pointed. These changes suggest that the right ventricle is stiffer in older subjects, with less dynamic contraction of the RVIT and less bellows-like movement.
Conclusions: This study established normal three-dimensional echocardiographic values for RV rCI, which are needed to further study RV diastolic dysfunction and remodeling with disease.
Keywords: Curvature; Normal heart; Right ventricle; Three-dimensional echocardiography.
Copyright © 2017 American Society of Echocardiography. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Conflicts of Interest: None.
Figures






References
-
- Ryan T, Petrovic O, Dillon JC, Feigenbaum H, Conley MJ, Armstrong WF. An echocardiographic index for separation of right ventricular volume and pressure overload. J Am Coll Cardiol. 1985;5:918–27. - PubMed
-
- Sheehan FH, Ge S, Vick GW, III, Urnes K, Kerwin WS, Bolson EL, et al. Three-dimensional shape analysis of right ventricular remodeling in repaired tetralogy of Fallot. Am J Cardiol. 2008;101:107–13. - PubMed
-
- Kang DK, Thilo C, Schoepf UJ, Barraza JM, Jr, Nance JW, Jr, Bastarrika G, et al. CT signs of right ventricular dysfunction: prognostic role in acute pulmonary embolism. JACC Cardiovasc Imaging. 2011;4:841–9. - PubMed
-
- Topilsky Y, Khanna A, Le Tourneau T, Park S, Michelena H, Suri R, et al. Clinical context and mechanism of functional tricuspid regurgitation in patients with and without pulmonary hypertension. Circ Cardiovasc Imaging. 2012;5:314–23. - PubMed
-
- Maffessanti F, Lang RM, Corsi C, Mor-Avi V, Caiani EG. Feasibility of left ventricular shape analysis from transthoracic real-time 3-D echocardiographic images. Ultrasound Med Biol. 2009;35:1953–62. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
