

Chromatin organisation and cancer prognosis: a pan-cancer study
- PMID: 29402700
- PMCID: PMC5842159
- DOI: 10.1016/S1470-2045(17)30899-9
Chromatin organisation and cancer prognosis: a pan-cancer study
Abstract
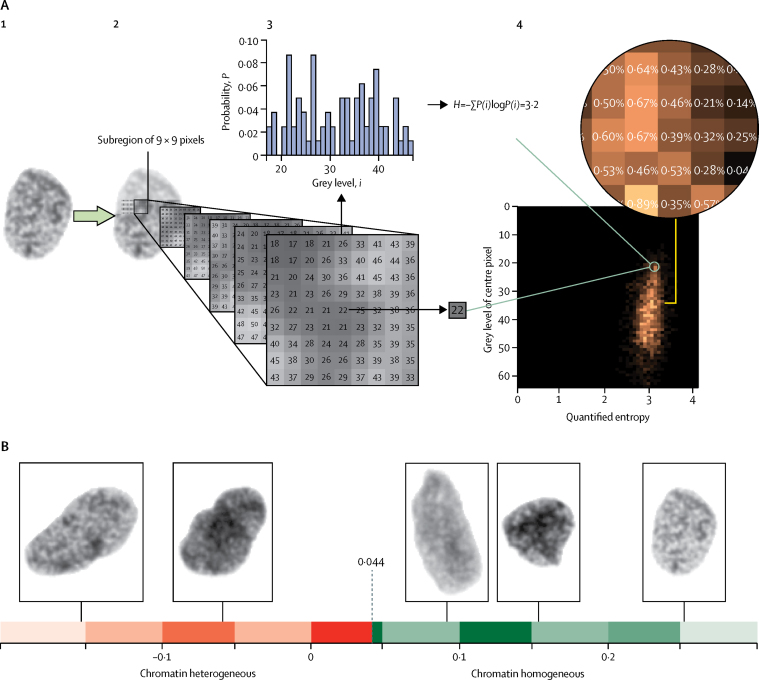
Background: Chromatin organisation affects gene expression and regional mutation frequencies and contributes to carcinogenesis. Aberrant organisation of DNA has been correlated with cancer prognosis in analyses of the chromatin component of tumour cell nuclei using image texture analysis. As yet, the methodology has not been sufficiently validated to permit its clinical application. We aimed to define and validate a novel prognostic biomarker for the automatic detection of heterogeneous chromatin organisation.
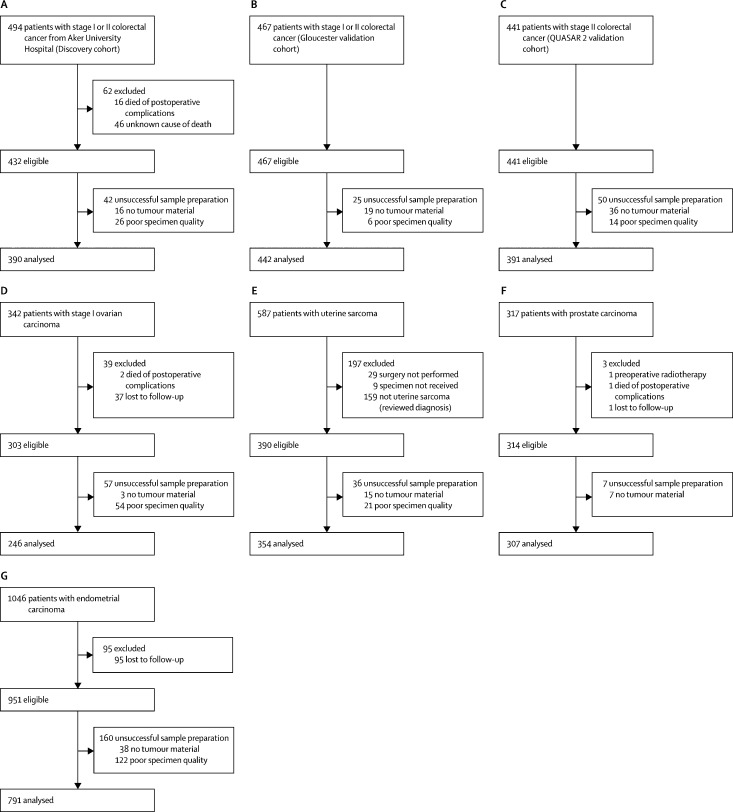
Methods: Machine learning algorithms analysed the chromatin organisation in 461 000 images of tumour cell nuclei stained for DNA from 390 patients (discovery cohort) treated for stage I or II colorectal cancer at the Aker University Hospital (Oslo, Norway). The resulting marker of chromatin heterogeneity, termed Nucleotyping, was subsequently independently validated in six patient cohorts: 442 patients with stage I or II colorectal cancer in the Gloucester Colorectal Cancer Study (UK); 391 patients with stage II colorectal cancer in the QUASAR 2 trial; 246 patients with stage I ovarian carcinoma; 354 patients with uterine sarcoma; 307 patients with prostate carcinoma; and 791 patients with endometrial carcinoma. The primary outcome was cancer-specific survival.
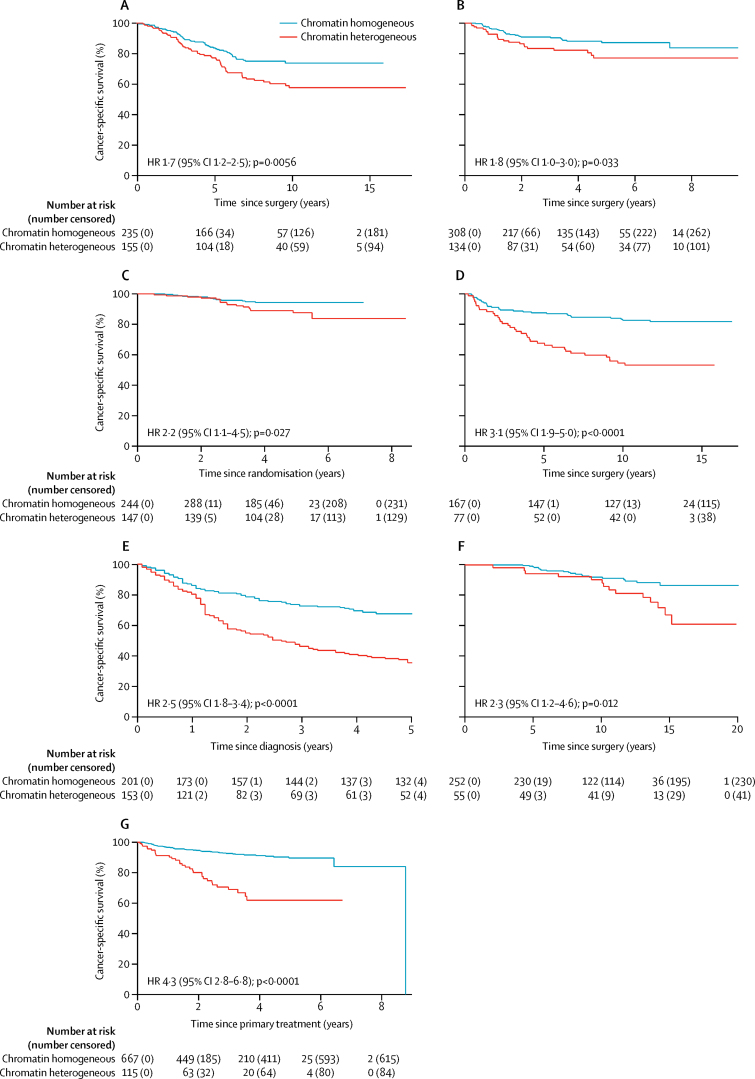
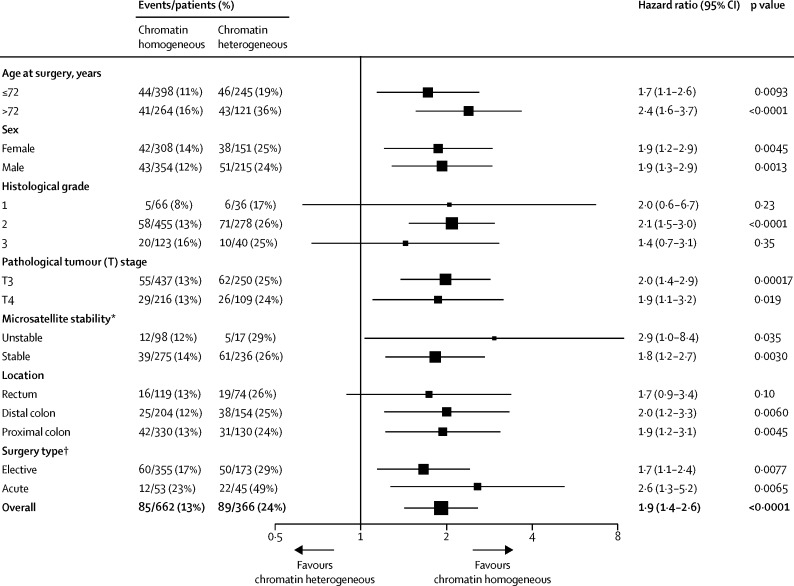
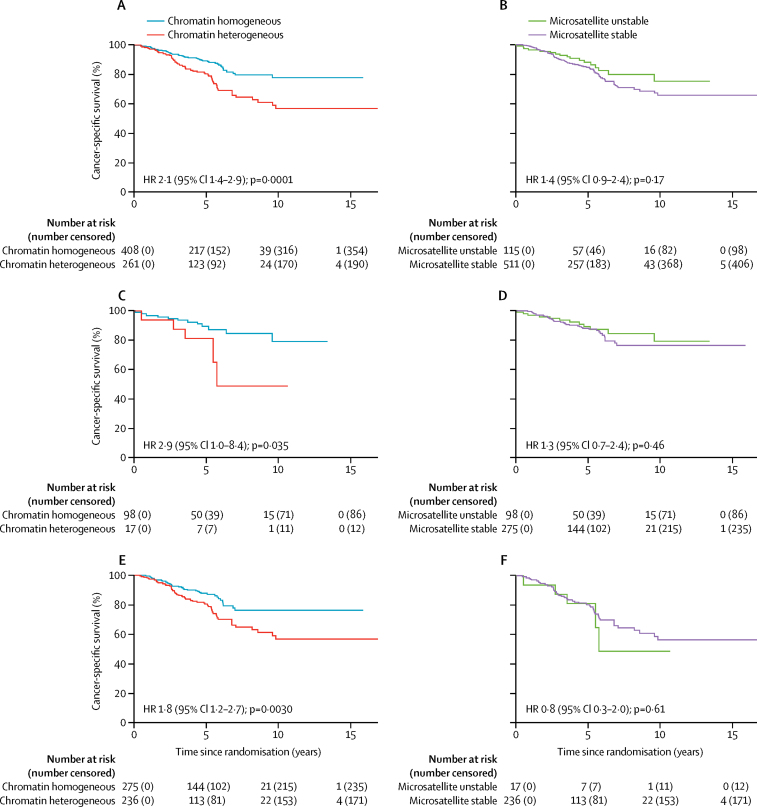
Findings: In all patient cohorts, patients with chromatin heterogeneous tumours had worse cancer-specific survival than patients with chromatin homogeneous tumours (univariable analysis hazard ratio [HR] 1·7, 95% CI 1·2-2·5, in the discovery cohort; 1·8, 1·0-3·0, in the Gloucester validation cohort; 2·2, 1·1-4·5, in the QUASAR 2 validation cohort; 3·1, 1·9-5·0, in the ovarian carcinoma cohort; 2·5, 1·8-3·4, in the uterine sarcoma cohort; 2·3, 1·2-4·6, in the prostate carcinoma cohort; and 4·3, 2·8-6·8, in the endometrial carcinoma cohort). After adjusting for established prognostic patient characteristics in multivariable analyses, Nucleotyping was prognostic in all cohorts except for the prostate carcinoma cohort (HR 1·7, 95% CI 1·1-2·5, in the discovery cohort; 1·9, 1·1-3·2, in the Gloucester validation cohort; 2·6, 1·2-5·6, in the QUASAR 2 cohort; 1·8, 1·1-3·0, for ovarian carcinoma; 1·6, 1·0-2·4, for uterine sarcoma; 1·43, 0·68-2·99, for prostate carcinoma; and 1·9, 1·1-3·1, for endometrial carcinoma). Chromatin heterogeneity was a significant predictor of cancer-specific survival in microsatellite unstable (HR 2·9, 95% CI 1·0-8·4) and microsatellite stable (1·8, 1·2-2·7) stage II colorectal cancer, but microsatellite instability was not a significant predictor of outcome in chromatin homogeneous (1·3, 0·7-2·4) or chromatin heterogeneous (0·8, 0·3-2·0) stage II colorectal cancer.
Interpretation: The consistent prognostic prediction of Nucleotyping in different biological and technical circumstances suggests that the marker of chromatin heterogeneity can be reliably assessed in routine clinical practice and could be used to objectively assist decision making in a range of clinical settings. An immediate application would be to identify high-risk patients with stage II colorectal cancer who might have greater absolute benefit from adjuvant chemotherapy. Clinical trials are warranted to evaluate the survival benefit and cost-effectiveness of using Nucleotyping to guide treatment decisions in multiple clinical settings.
Funding: The Research Council of Norway, the South-Eastern Norway Regional Health Authority, the National Institute for Health Research, and the Wellcome Trust.
Copyright © 2018 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC-BY-NC-ND 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Figures
Comment in
-
Next-generation nuclear morphology to grade solid tumours.Lancet Oncol. 2018 Mar;19(3):275-277. doi: 10.1016/S1470-2045(18)30063-9. Epub 2018 Feb 3. Lancet Oncol. 2018. PMID: 29402699 No abstract available.
References
-
- Lengauer C, Kinzler KW, Vogelstein B. Genetic instabilities in human cancers. Nature. 1998;396:643–649. - PubMed
-
- Danielsen HE, Pradhan M, Novelli M. Revisiting tumour aneuploidy—the place of ploidy assessment in the molecular era. Nat Rev Clin Oncol. 2016;13:291–304. - PubMed
-
- Schuster-Böckler B, Lehner B. Chromatin organization is a major influence on regional mutation rates in human cancer cells. Nature. 2012;488:504–507. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
