

Hospital Readmission among New Dialysis Patients Associated with Young Age and Poor Functional Status
- PMID: 29402792
- PMCID: PMC5920698
- DOI: 10.1159/000485985
Hospital Readmission among New Dialysis Patients Associated with Young Age and Poor Functional Status
Abstract
Background/aims: Over one-third of hospital discharges among dialysis patients are followed by 30-day readmission. The first year after dialysis start is a high-risk time frame. We examined the rate, causes, timing, and predictors of 30-day readmissions among adult, incident dialysis patients.
Methods: Hospital readmissions were assessed from the 91st day to the 15th month after the initiation of dialysis using a Mayo Clinic registry linkage to United States Renal Data System claims during the period January 2001-December 2010.
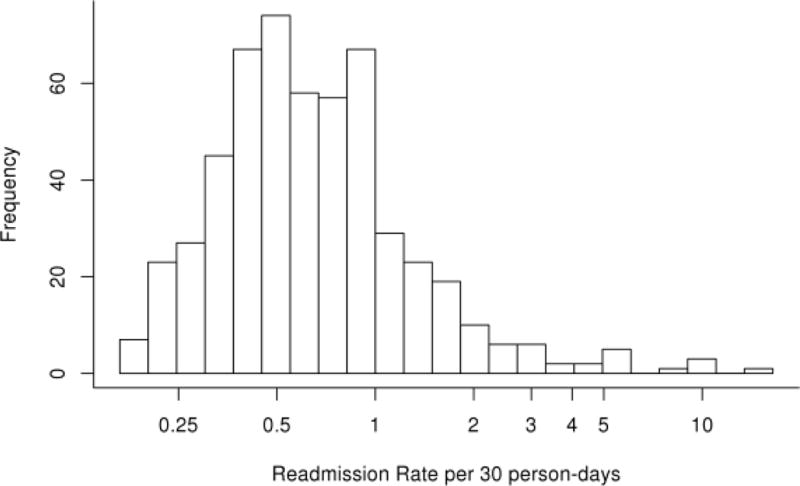
Results: Among 1,727 patients with ≥1 hospitalization, 532 (31%) had ≥1, and 261 (15%) had ≥2 readmissions. Readmission rate was 1.1% per person-day post-discharge, and the highest rates (2.5% per person-day) occurred ≤5 days after index admission. The overall cumulative readmission rate was 33.8% at day 30. Common readmission diagnoses included cardiac issues (22%), vascular disorders (19%), and infection (13%). Similar-cause readmissions to index hospitalization were more common during days 0-14 post-discharge than days 15-30 (37.5 vs. 22.9%; p = 0.004). Younger age at dialysis initiation, inability to transfer/ambulate, serum creatinine ≤5.3 mg/dL, higher number of previous hospitalizations, and longer duration on dialysis were associated with higher readmission rates in multivariable analyses. Patients aged 18-39 were few (8.3%) but comprised 17.7% of "high-readmission" users such that a 30-year-old patient had an 87% chance of being readmitted within 30 days of any hospital discharge, whereas an 80-year-old patient had a 25% chance.
Conclusions: Overall, 30-day readmissions are common within the first year of dialysis start. The first 10-day period after discharge, young patients, and those with poor functional status represent key areas for targeted interventions to reduce readmissions.
Keywords: Hospitalization; Cardiovascular disease; Death; Heart failure; Hemodialysis; Mortality; Youth.
© 2018 S. Karger AG, Basel.
Conflict of interest statement
The authors report no competing financial interests.
Disclosure: A.W.W. American Society of Nephrology Public Policy Board
Figures






References
-
- USRDS. United States Renal Data System 2014 Annual Data Report: Atlas of Chronic Kidney Disease and End-Stage Renal Disease in the United States, National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases. Bethesda, MD: Bethesda; 2014.
-
- CMS. Centers for Medicare and Medicaid Services, ESRD Quality Incentive Program. End-Stage Renal Disease (ESRD) Quality Incentive Program (QIP) promotes high-quality services in outpatient dialysis facilities treating patients with ESRD. 2015 Available at: http://www.cms.gov/Medicare/Quality-Initiatives-Patient-Assessment-Instr... 2015.
-
- CMS. Centers for Medicare and Medicaid Services, Readmissions Reduction Program. 2015 http://www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/AcuteInpati.... Accessed 3/2/15, 2015.
-
- Centers for Medicaid and Medicare Services (CMS) Report for the Standardized Readmission Ratio, ESRD Quality Measure Development, Maintenance, and Support. 2014 http://www.cms.gov/Medicare/Quality-Initiatives-Patient-Assessment-Instr....
-
- CMS. Centers for Medicare and Medicaid Services, ESRD Quality Incentive Program (QIP) End-Stage Renal Disease (ESRD) Quality Incentive Program (QIP) promotes high-quality services in outpatient dialysis facilities treating patients with ESRD. 2016 Available at: https://www.cms.gov/Medicare/Quality-Initiatives-Patient-Assessment-Inst.... 2017.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
