

CLCN2 chloride channel mutations in familial hyperaldosteronism type II
- PMID: 29403011
- PMCID: PMC5862758
- DOI: 10.1038/s41588-018-0048-5
CLCN2 chloride channel mutations in familial hyperaldosteronism type II
Abstract
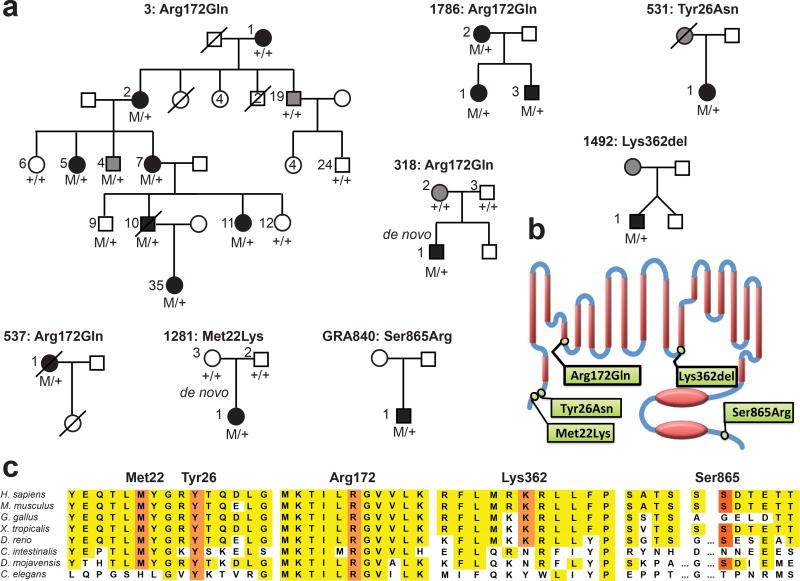
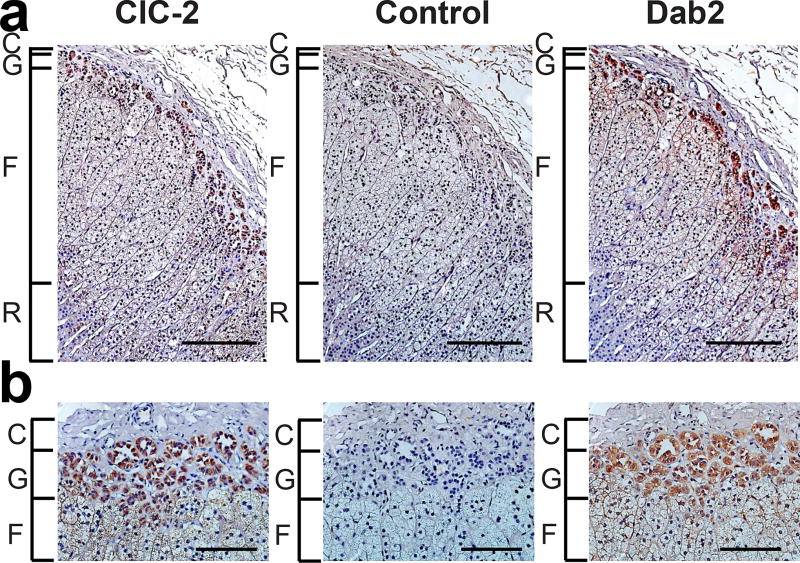
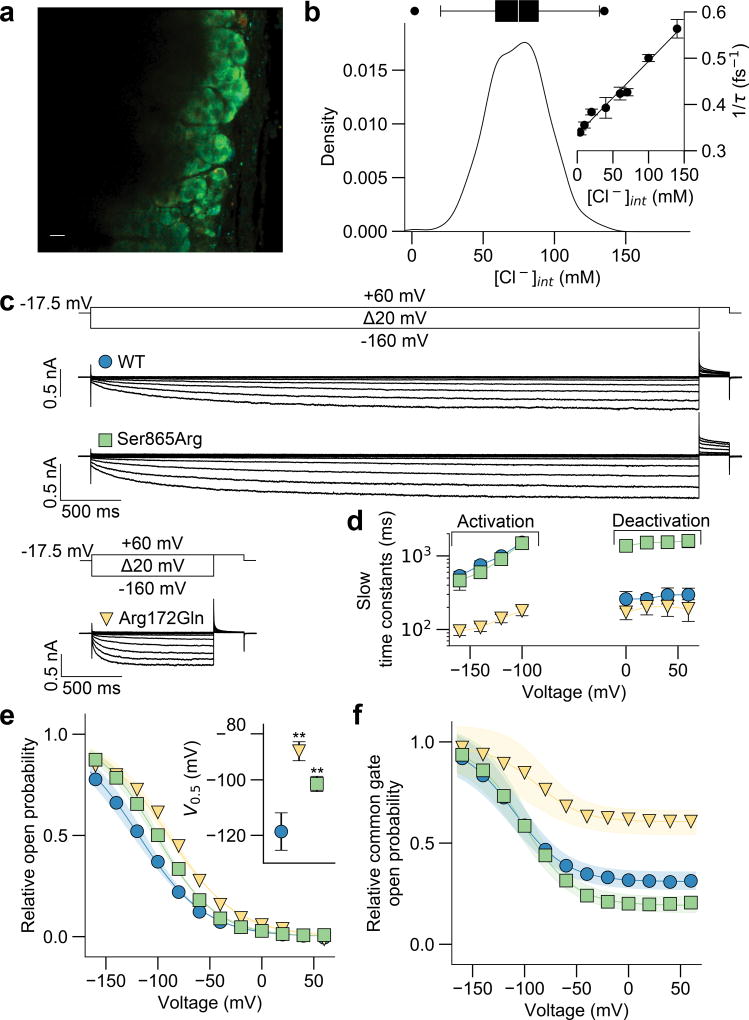
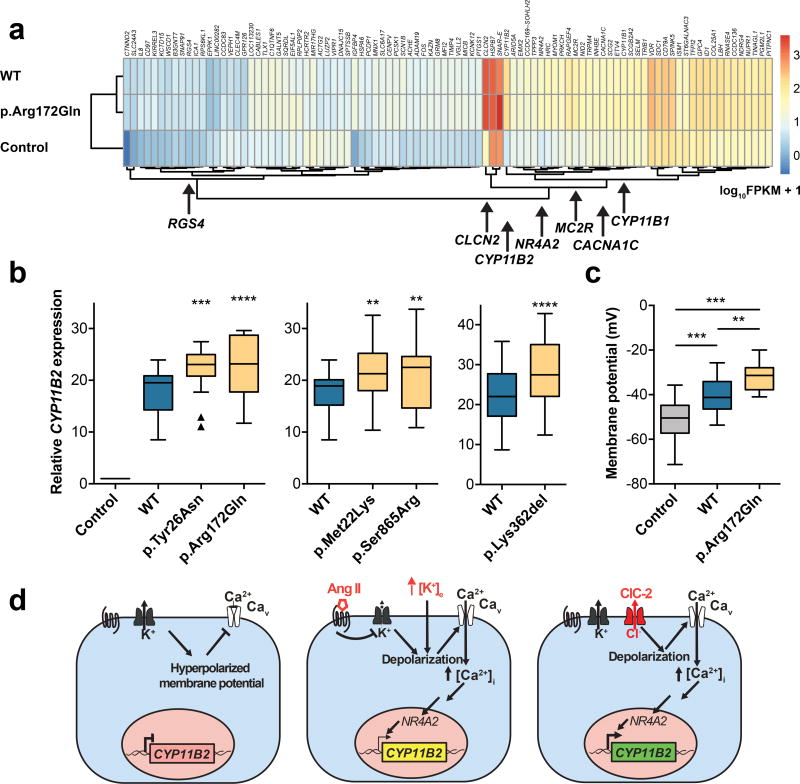
Primary aldosteronism, a common cause of severe hypertension 1 , features constitutive production of the adrenal steroid aldosterone. We analyzed a multiplex family with familial hyperaldosteronism type II (FH-II) 2 and 80 additional probands with unsolved early-onset primary aldosteronism. Eight probands had novel heterozygous variants in CLCN2, including two de novo mutations and four independent occurrences of a mutation encoding an identical p.Arg172Gln substitution; all relatives with early-onset primary aldosteronism carried the CLCN2 variant found in the proband. CLCN2 encodes a voltage-gated chloride channel expressed in adrenal glomerulosa that opens at hyperpolarized membrane potentials. Channel opening depolarizes glomerulosa cells and induces expression of aldosterone synthase, the rate-limiting enzyme for aldosterone biosynthesis. Mutant channels show gain of function, with higher open probabilities at the glomerulosa resting potential. These findings for the first time demonstrate a role of anion channels in glomerulosa membrane potential determination, aldosterone production and hypertension. They establish the cause of a substantial fraction of early-onset primary aldosteronism.
Conflict of interest statement
Heinrich Heine University Düsseldorf has filed a patent application: EP17209972, Diagnosis and Therapy of Primary Aldosteronism.
Figures
Comment in
-
Hypertension: CLCN2 chloride channel mutations in primary aldosteronism.Nat Rev Nephrol. 2018 Apr;14(4):213. doi: 10.1038/nrneph.2018.17. Epub 2018 Feb 26. Nat Rev Nephrol. 2018. PMID: 29479080 No abstract available.
References
-
- Monticone S, et al. Prevalence and Clinical Manifestations of Primary Aldosteronism Encountered in Primary Care Practice. J Am Coll Cardiol. 2017;69:1811–1820. - PubMed
-
- Stowasser M, et al. Familial hyperaldosteronism type II: five families with a new variety of primary aldosteronism. Clin Exp Pharmacol Physiol. 1992;19:319–22. - PubMed
-
- Funder JW, et al. The Management of Primary Aldosteronism: Case Detection, Diagnosis, and Treatment: An Endocrine Society Clinical Practice Guideline. J Clin Endocrinol Metab. 2016;101:1889–916. - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
Miscellaneous
