

Pain associated with health and economic burden in France: results from recent National Health and Wellness Survey data
- PMID: 29403296
- PMCID: PMC5779295
- DOI: 10.2147/CEOR.S148405
Pain associated with health and economic burden in France: results from recent National Health and Wellness Survey data
Abstract
Purpose: This study aimed to estimate the prevalence of pain among French adults and assess the impact of pain on health-related quality of life (HRQoL), activity impairment, and health care resource use (HRU).
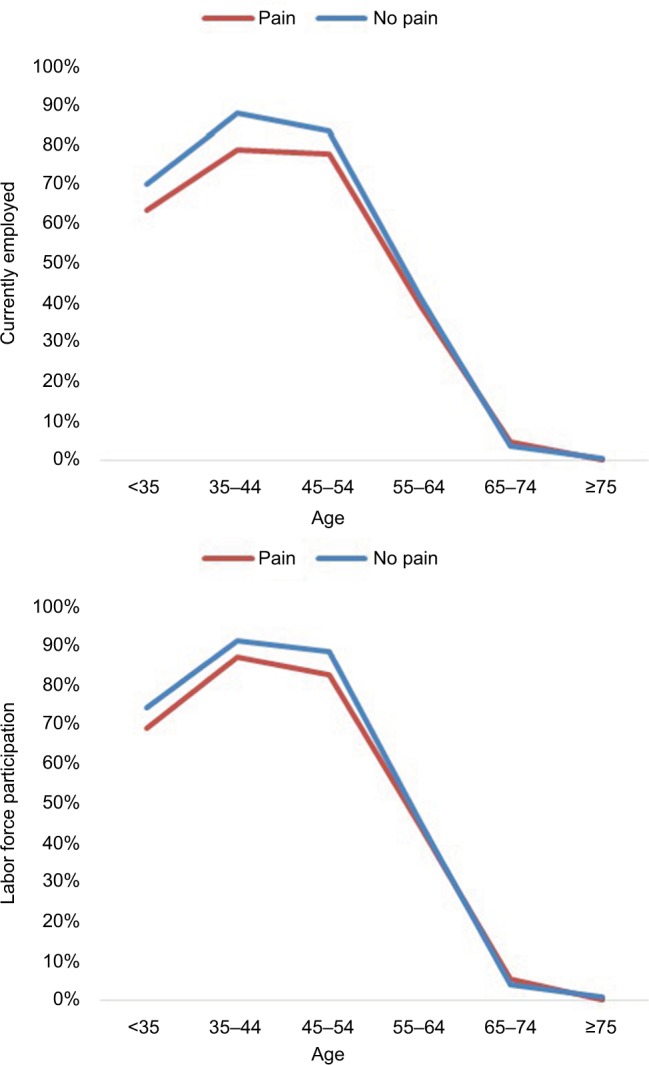
Patients and methods: Respondents from the 2015 France National Health and Wellness Survey (N=19,173) were categorized by self-reported pain (experienced pain in the past 12 months vs no pain) and compared on HRQoL (36-Item Short Form Health Survey version 2: Mental Component Summary, Physical Component Summary, and Short Form-6 Dimensions health utilities), activity impairment (Work Productivity and Activity Impairment questionnaire), employment status, and HRU (health care provider visits, emergency room visits, and hospitalizations). Bivariate analyses examined differences between pain groups stratified by age, sex, income, and Charlson comorbidity index (CCI) scores.
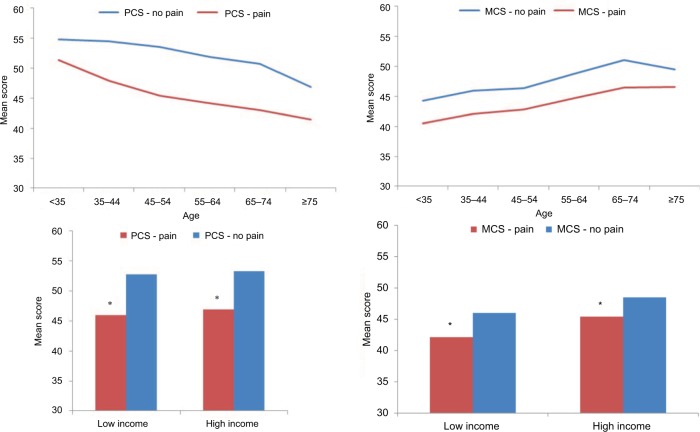
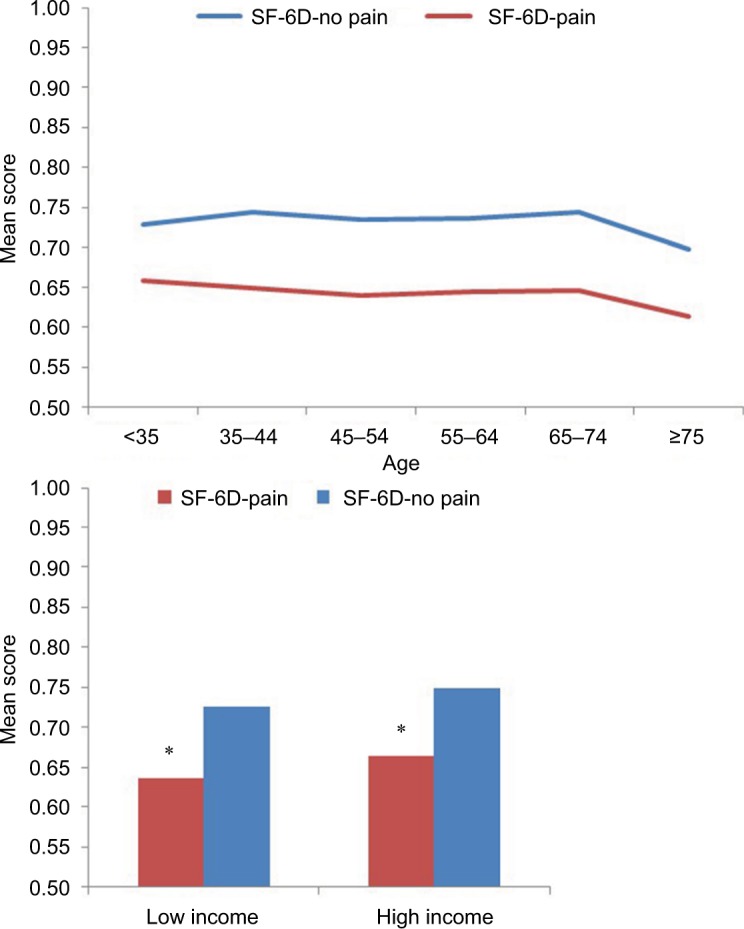
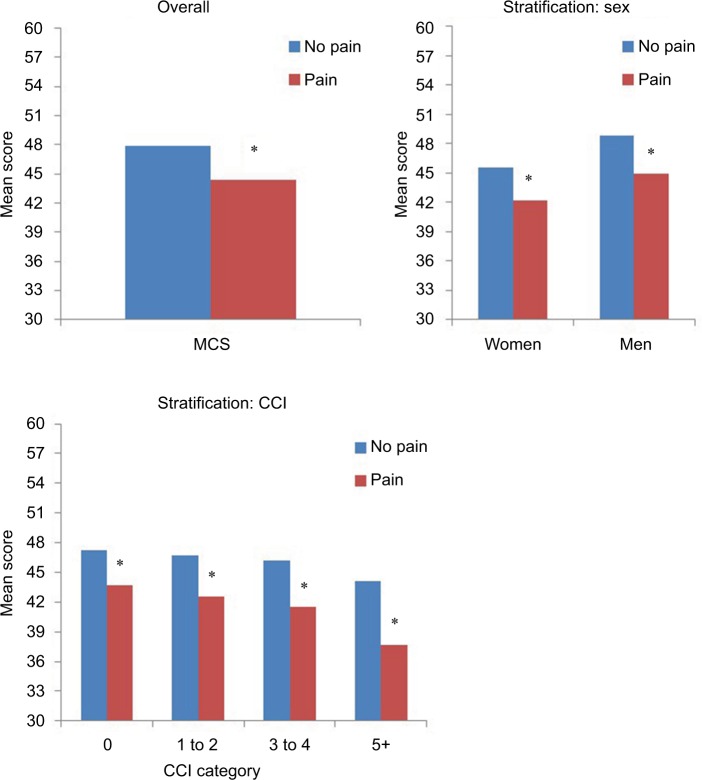
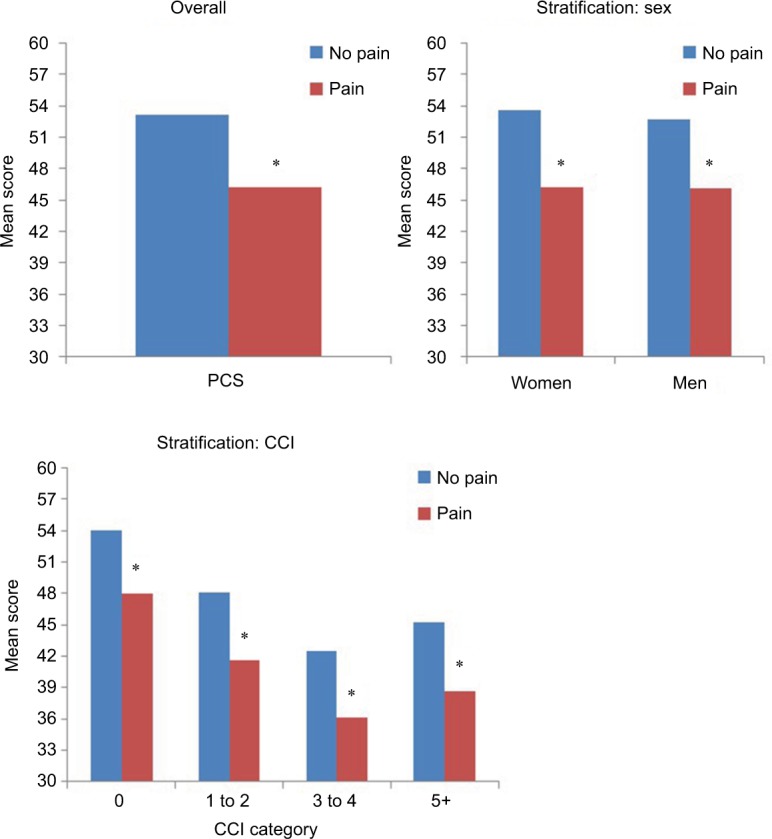
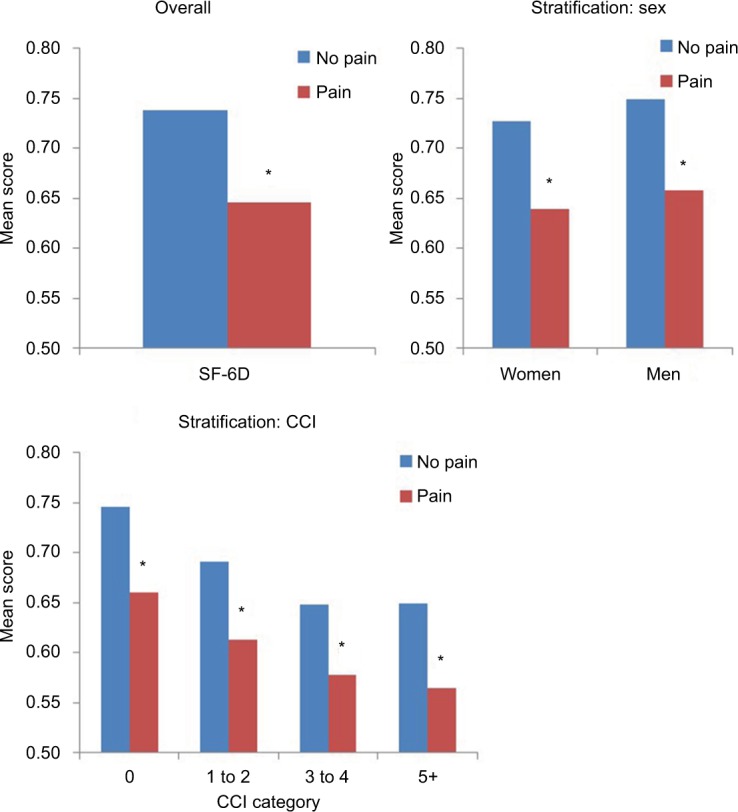
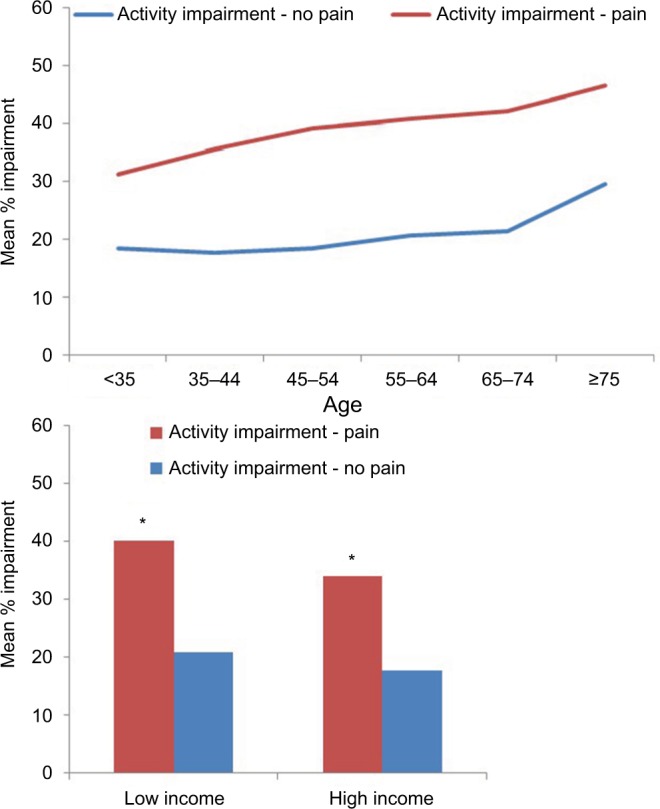
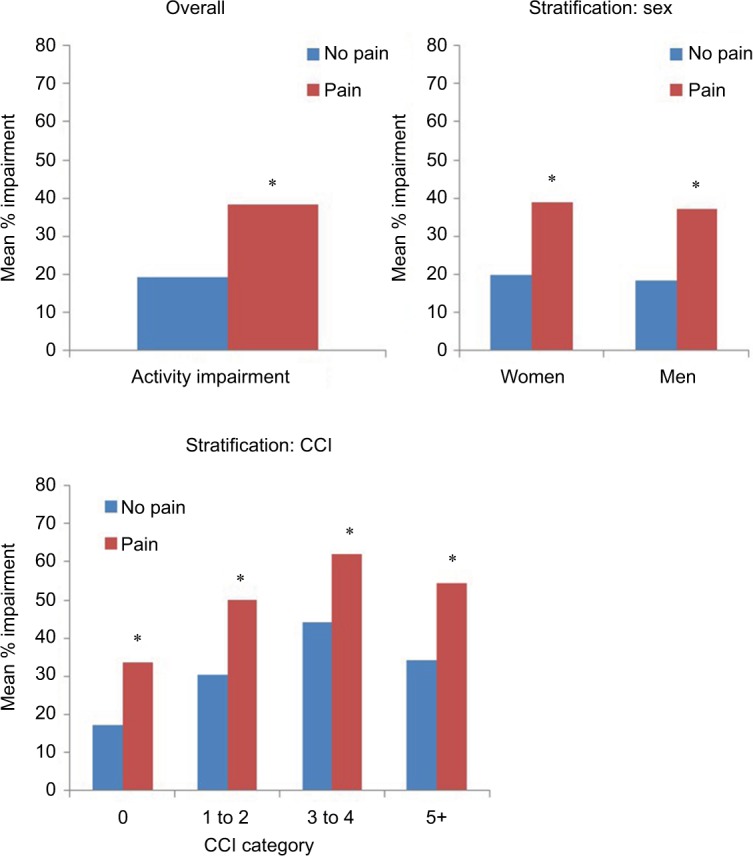
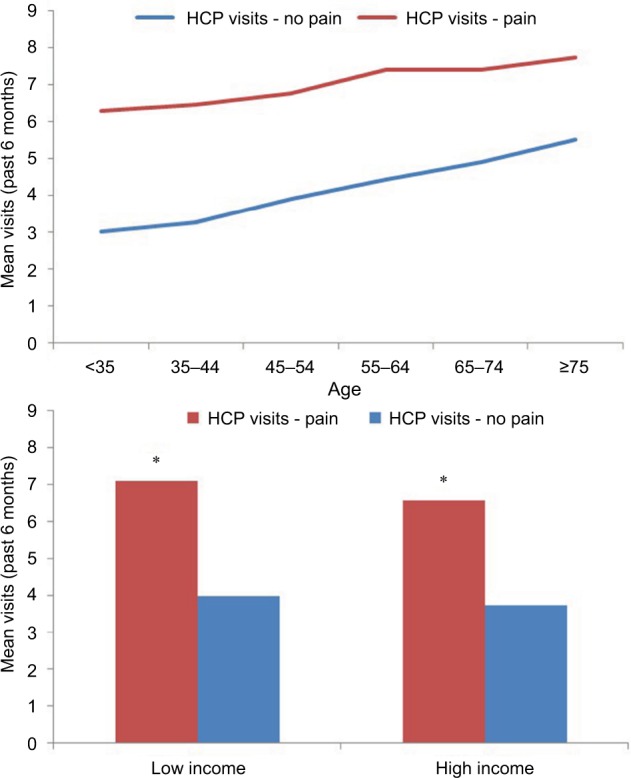
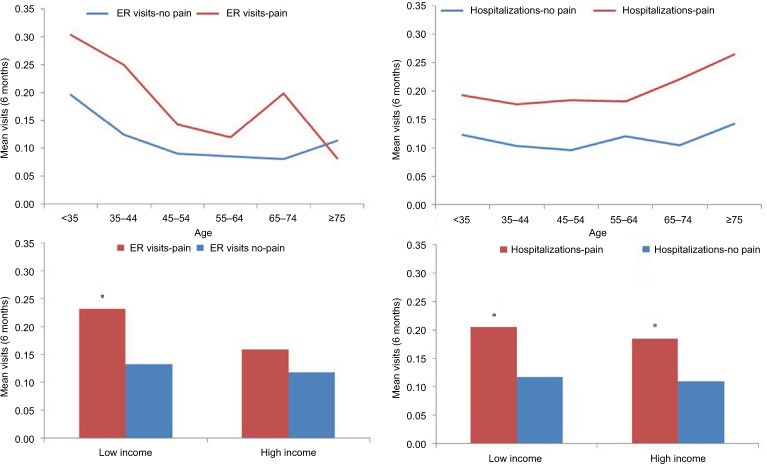
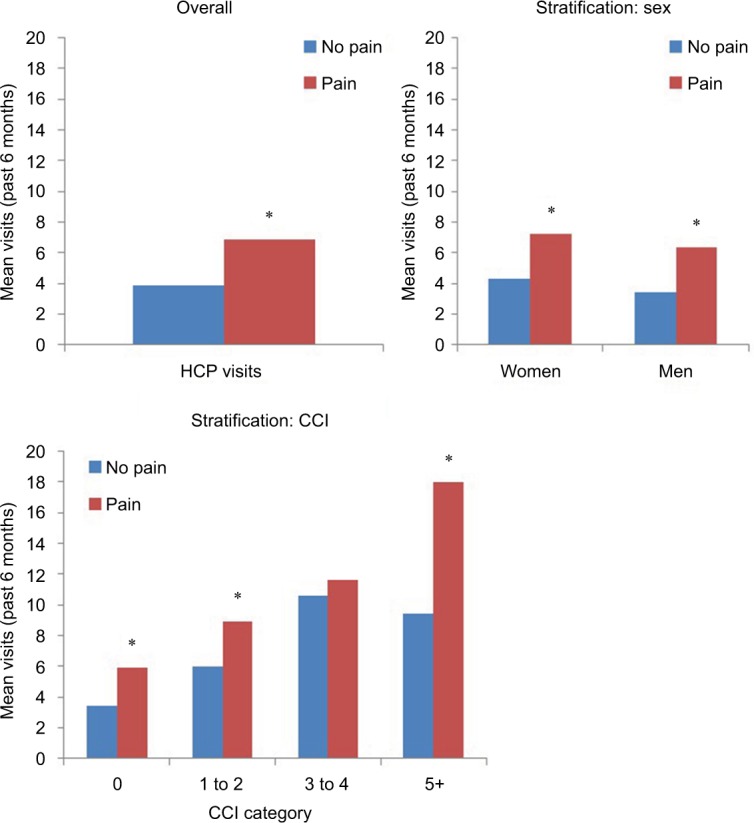
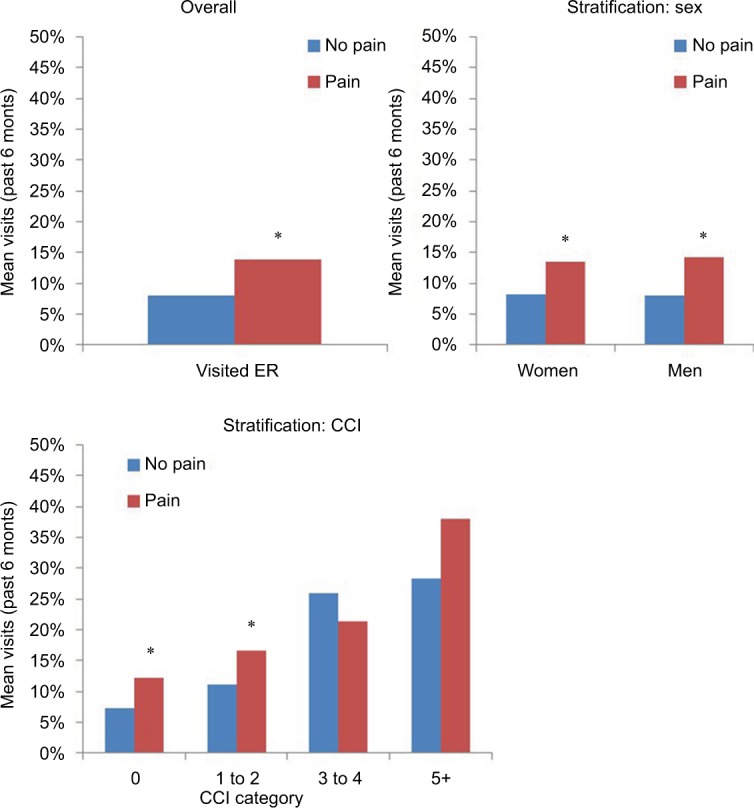
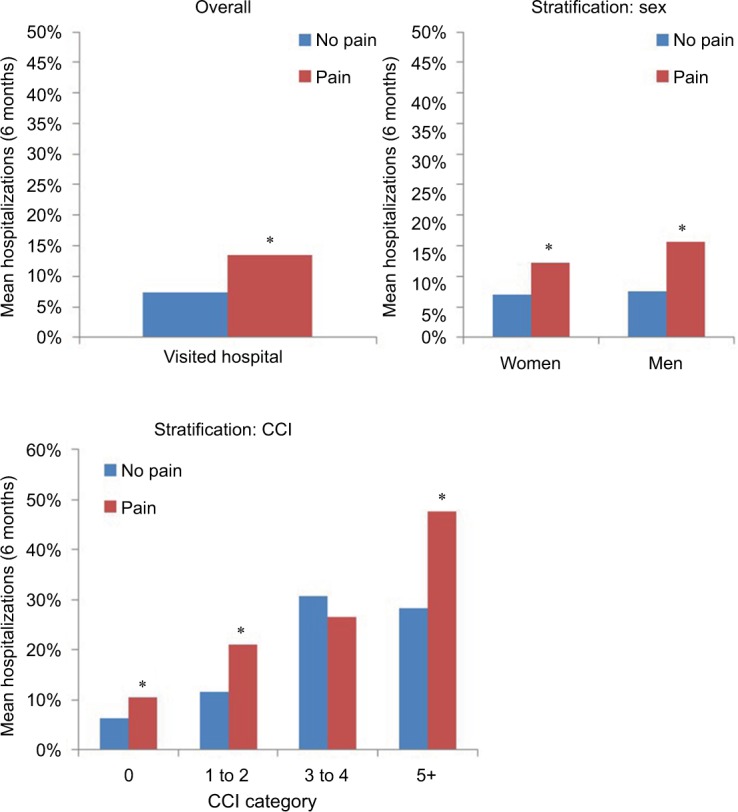
Results: Pain prevalence was 20.2% (n=4007). Mean Physical Component Summary decrements with pain ranged from 3.4 to 8.1 points among those aged <35 years to those aged 45-54 years, respectively. Results for Mental Component Summary and Short Form-6 Dimensions scores followed similar patterns. Regardless of income, sex, or CCI group, pain was associated with significant decrements on all HRQoL measures (for all, p<0.05). The impact of pain on activity impairment was lowest among those <35 years; this impact was higher in middle age and then tapered off among those aged ≥75 years. Pain was associated with greater activity impairment and more health care provider visits across income, sex, and CCI groups (for all, p<0.05). Generally, emergency room visits were more common among those with pain across age, sex, and CCI, but they were only significantly associated with pain in the lower income group (p<0.01). Pain was associated with significantly more hospitalizations across age and income groups.
Conclusion: Results suggest pain negatively affects HRQoL, activity impairment, and HRU across demographic subgroups. These findings help underscore the considerable health and economic burden of pain in France.
Keywords: activity impairment; health care resource use; health-related quality of life; prevalence.
Conflict of interest statement
Disclosure YH, BC, and LG are employees of Mundipharma. The authors report no other conflicts of interest in this work.
Figures

References
-
- Demyttenaere K, Bonnewyn A, Bruffaerts R, Brugh T, De Graaf R, Alonso J. Comorbid painful physical symptoms and depression: prevalence, work loss, and help seeking. J Affect Disord. 2006;92(2–3):185–193. - PubMed
-
- O’Brien T, Breivik H. The impact of chronic pain–European patients’ perspective over 12 months. Scand J Pain. 2012;3:23–29. - PubMed
-
- Goren A, Mould-Quevedo J, DiBonaventura MD. Prevalence of pain reporting and associated health outcomes across emerging markets and developed countries. Pain Med. 2014;15(11):1880–1891. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
