

Surgical approach to limiting skin contracture following protractor myectomy for essential blepharospasm
- PMID: 29403334
- PMCID: PMC5791625
- DOI: 10.5693/djo.01.2016.11.001
Surgical approach to limiting skin contracture following protractor myectomy for essential blepharospasm
Abstract
Purpose: To report our experience with protractor myectomy in patients with benign essential blepharospasm who did not respond to serial botulinum toxin injection, and to describe intra- and postoperative techniques that limited skin contracture while also providing excellent functional and cosmetic results.
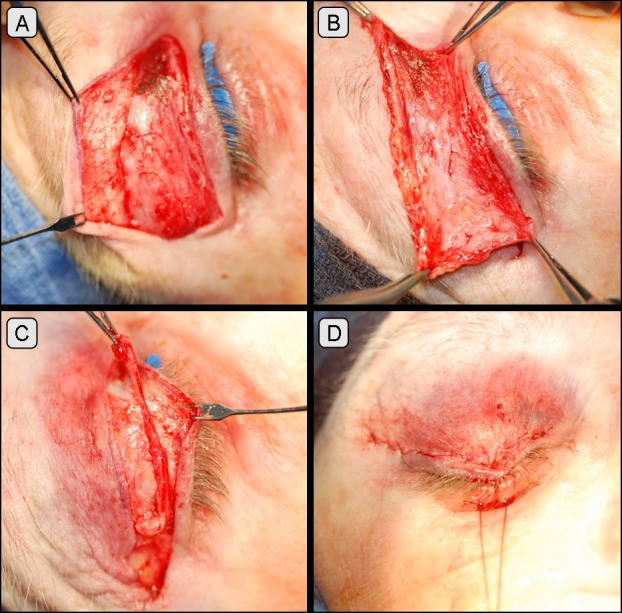
Methods: The medical records of patients with isolated, benign, essential blepharospasm who underwent protractor myectomy from 2005 to 2008 by a single surgeon were reviewed retrospectively. The technique entailed operating on a single eyelid during each procedure, using a complete en bloc resection of all orbicularis tissue, leaving all eyelid skin intact at the time of surgery, and placing the lid under stretch with Frost suture and applying a pressure dressing for 5-7 days.
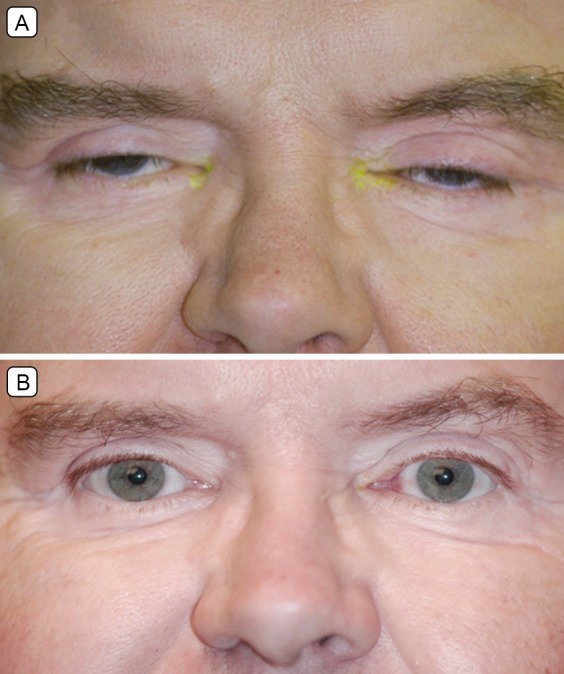
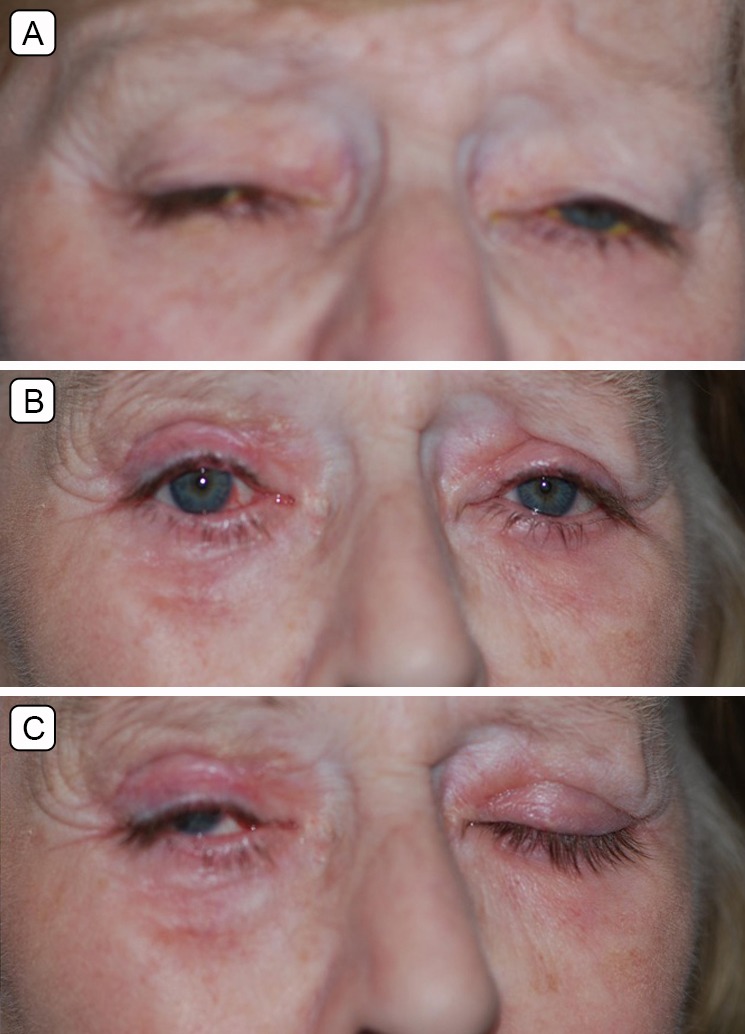
Results: Data from 28 eyelids in 7 patients were included. Average follow-up was 21.5 months (range, 4-76 months). Of the 28 eyelids, 20 (71.4%) showed postoperative resolution of spasm, with no further need for botulinum toxin injections. In the 8 eyelids requiring further injections, the average time to injection after surgery was 194 days (range, 78-323 days), and the average number of injections was 12 (range, 2-23 injections). All but one eyelid had excellent cosmetic results, without signs of contracture; one eyelid developed postoperative skin contracture following premature removal of the Frost suture and pressure dressing because of concerns over increased intraocular pressure.
Conclusions: In our patient cohort, this modified technique resulted in excellent cosmetic and functional results and limited postoperative skin contracture.
Figures
Similar articles
-
Follow-up of patients with essential blepharospasm who underwent eyelid protractor myectomy at the Mayo Clinic from 1980 through 1995.Ophthalmic Plast Reconstr Surg. 1999 Mar;15(2):106-10. doi: 10.1097/00002341-199903000-00007. Ophthalmic Plast Reconstr Surg. 1999. PMID: 10189637
-
Skin contracture following upper eyelid orbiculectomy: is primary skin excision advisable?Orbit. 2013 Apr;32(2):107-10. doi: 10.3109/01676830.2013.771681. Orbit. 2013. PMID: 23565764
-
Orbicularis oculi muscle graft augmentation after protractor myectomy in blepharospasm.Ophthalmic Plast Reconstr Surg. 2003 Jul;19(4):287-96. doi: 10.1097/01.IOP.0000075020.81386.D5. Ophthalmic Plast Reconstr Surg. 2003. PMID: 12878877
-
Myectomy for blepharospasm 2013.Curr Opin Ophthalmol. 2013 Sep;24(5):488-93. doi: 10.1097/ICU.0b013e3283645aee. Curr Opin Ophthalmol. 2013. PMID: 23925062 Review.
-
Surgical Myectomy for Essential Blepharospasm and Hemifacial Spasm.Int Ophthalmol Clin. 2018 Winter;58(1):63-70. doi: 10.1097/IIO.0000000000000206. Int Ophthalmol Clin. 2018. PMID: 29239878 Review. No abstract available.
Cited by
-
Impact of Upper Eyelid Surgery on Symptom Severity and Frequency in Benign Essential Blepharospasm.J Mov Disord. 2021 Jan;14(1):53-59. doi: 10.14802/jmd.20075. Epub 2021 Jan 12. J Mov Disord. 2021. PMID: 33423436 Free PMC article.
References
-
- Bradley EA, Hodge DO, Bartley GB. Benign essential blepharospasm among residents of Olmsted County, Minnesota, 1976 to 1995: an epidemiologic study. Ophthal Plast Reconstr Surg. 2003;19:177–81. - PubMed
-
- Defazio G, Livrea P, De Salvia R, et al. Prevalence of primary blepharospasm in a community of Puglia region, Southern Italy. Neurology. 2001;156:1579–81. - PubMed
-
- Defazio G, Livrea P. Epidemiology of primary blepharospasm. Mov Disord. 2002;17:7–12. - PubMed
-
- Barnes MP, Best D, Kidd L. The use of botulinum toxin type-B in the treatment of patients who have become unresponsive to botulinum toxin type-A—initial experiences. Eur J Neurol. 2005;12:947–55. - PubMed
-
- Bhidayasiri R, Cardoso F, Truong DD. Botulinum toxin in blepharospasm and oromandibular dystonia: comparing different botulinum toxin preparations. Eur J Neurol. 2006;13:21–9. - PubMed
MeSH terms
Supplementary concepts
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials