

When myasthenia gravis is deemed refractory: clinical signposts and treatment strategies
- PMID: 29403543
- PMCID: PMC5791553
- DOI: 10.1177/1756285617749134
When myasthenia gravis is deemed refractory: clinical signposts and treatment strategies
Erratum in
-
Corrigendum.Ther Adv Neurol Disord. 2018 Mar 21;11:1756286418765591. doi: 10.1177/1756286418765591. eCollection 2018. Ther Adv Neurol Disord. 2018. PMID: 29595827 Free PMC article.
Abstract
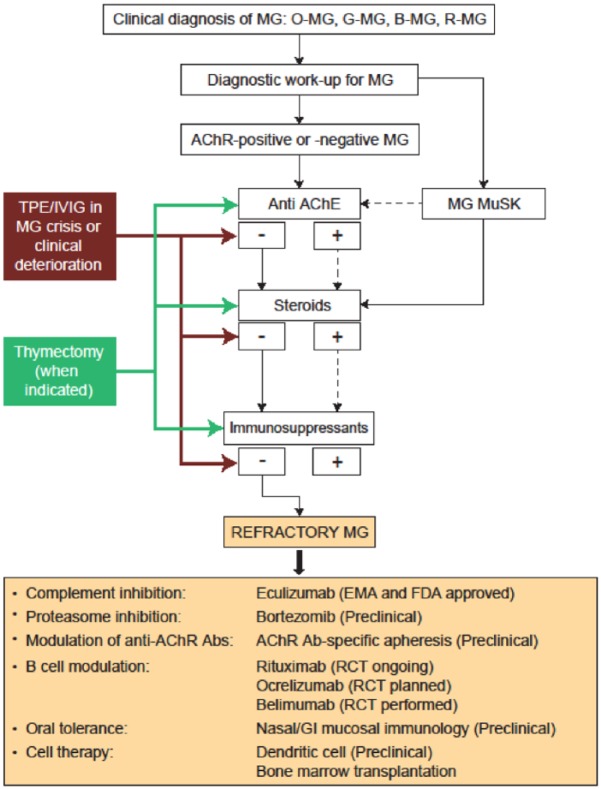
The prognosis for patients with myasthenia gravis (MG) has improved significantly over the past half century, including substantial reductions in mortality and morbidity. However, approximately 10% of patients fails to respond adequately to current therapies and are considered treatment refractory, or treatment intolerant, and up to 80% have disease that fails to achieve complete stable remission. Although patients with autoantibodies to muscle-specific tyrosine kinase (anti-MuSK positive) are more likely to become treatment refractory than those with autoantibodies to the acetylcholine receptor (anti-AChR positive), each of these serotypes is substantially represented in the refractory MG population. Other risk factors for becoming treatment refractory include history of thymoma or thymectomy and female sex. A modified treatment algorithm for MG is proposed: patients who have disease that fails to respond to the stepwise approach to therapy, are treatment intolerant, or who require chronic rescue measures despite ongoing therapy, should be considered treatment refractory and emerging therapies should be considered. Three emerging monoclonal antibody-based therapies are discussed: the anti-B-cell agent rituximab; the terminal complement activation inhibitor eculizumab; and belimumab, which targets B-cell activating factor. Increased understanding of molecular pathophysiology and accurate antibody subtyping in MG should lead to the use of new therapeutic agents and successful management of treatment-refractory patients.
Keywords: acetylcholine receptor antibodies; monoclonal antibodies; muscle-specific tyrosine kinase antibodies; myasthenia gravis; treatment intolerant; treatment refractory.
Conflict of interest statement
Conflict of interest statement: R. Mantegazza has received honoraria from Alexion Pharmaceuticals, Inc. (New Haven, CT, USA). C. Antozzi received no financial support for the research, authorship, and/or publication of this article.
Figures
References
-
- Spillane J, Higham E, Kullmann DM. Myasthenia gravis. BMJ 2012; 345: e8497. - PubMed
-
- Li Y, Arora Y, Levin K. Myasthenia gravis: newer therapies offer sustained improvement. Cleve Clin J Med 2013; 80: 711–721. - PubMed
-
- Grob D, Brunner N, Namba T, et al. Lifetime course of myasthenia gravis. Muscle Nerve 2008; 37: 141–149. - PubMed
-
- Grob D, Brunner NG, Namba T. The natural course of myasthenia gravis and effect of therapeutic measures. Ann N Y Acad Sci 1981; 377: 652–669. - PubMed
-
- Baggi F, Andreetta F, Maggi L, et al. Complete stable remission and autoantibody specificity in myasthenia gravis. Neurology 2013; 80: 188–195. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
