

Review
doi: 10.1055/s-0037-1615810.
Epub 2018 Jan 18.
Juvenile Angiofibroma: Current Management Strategies
Affiliations
- PMID: 29404237
- PMCID: PMC5796815
- DOI: 10.1055/s-0037-1615810
Item in Clipboard
Review
Juvenile Angiofibroma: Current Management Strategies
J Neurol Surg B Skull Base.
2018 Feb.
Abstract
Juvenile angiofibroma (JA) is a benign, highly vascular tumor which is diagnosed on the basis of clinical and imaging features. It has a characteristic pattern of spread commonly involving the pterygopalatine fossa and pterygoid base. The mainstay of treatment is surgery, while radiotherapy is rarely used for the treatment of recurrent lesion. Endoscopic endonasal surgery is currently the treatment of choice for small to intermediate size JAs, and is feasible even for advanced lesions; however, this should only be practiced in well-experienced centers.
Keywords: endoscopic surgery; juvenile angiofibroma; surgical treatment of juvenile angiofibroma.
Figures
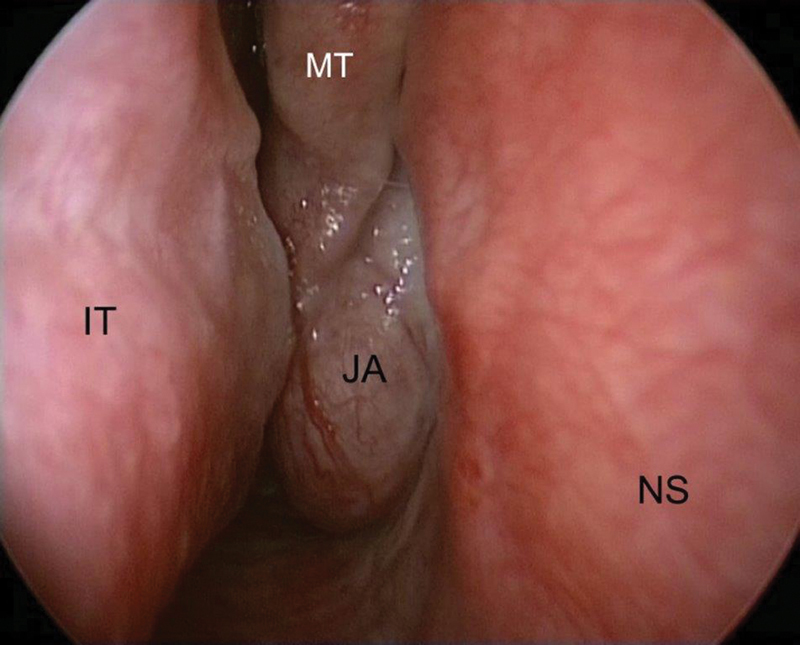
Endoscopic view of the right nasal fossa. Juvenile angiofibroma (JA) obstructing the nasal cavity and protruding between the middle turbinate (MT) and the nasal septum (NS). Abbreviation: IT, inferior turbinate.
(
A
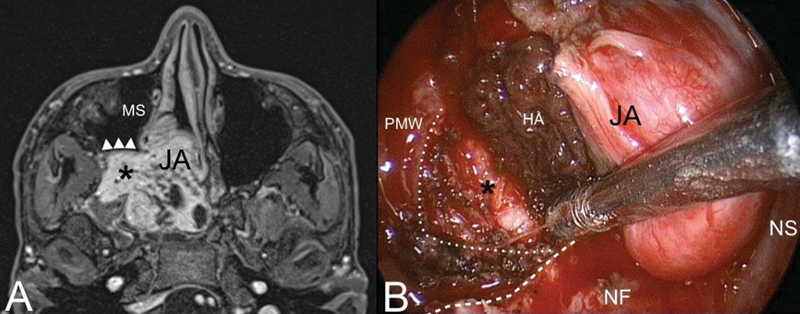
) Axial contrast-enhanced T1-weighted magnetic resonance (MR). Juvenile angiofibroma (JA) with typical extension into the pterygopalatine and infratemporal fossa (black asterisk). The posterior wall of the maxillary sinus (MS) is pushed forward by the lesion (white arrowheads). (
B
) Identification of the dissection plane cutting the posterior periosteum of the posterior maxillary wall (PMW) (white dotted line). Inferior turbinate and medial maxillary wall have been removed to adequately expose the posterior maxillary wall. White dashed line: inferior limit of the medial maxillary wall. Abbreviations: HA, hemostatic agent; NF, nasal floor; NS, nasal septum.
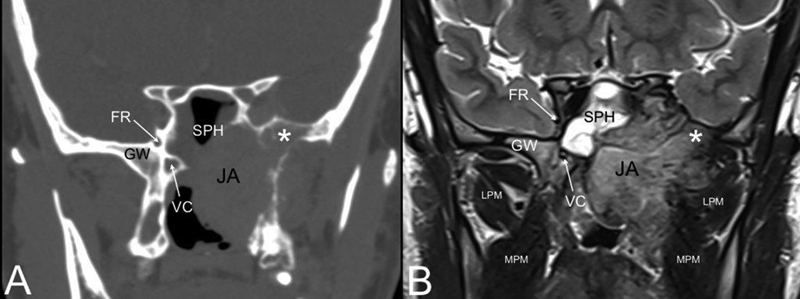
Coronal computed tomography (CT) (
A
) and T2-weighted magnetic resonance (MR) (
B
). Juvenile angiofibroma (JA) eroding the left greater wing (GW) of the sphenoid (white asterisk). Abbreviations: FR, foramen rotundum; LPM, lateral pterygoid muscle; MPM, medial pterygoid muscle; SPH, sphenoid sinus; VC, vidian canal.
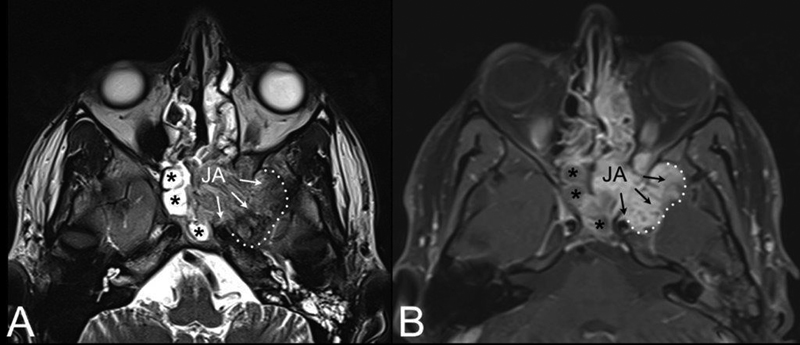
AxialT2-weighted (
A
) and contrast-enhanced T1-weighted magnetic resonance (MR) (
B
). Juvenile angiofibroma (JA) with intracranial extension (black arrows) into the middle cranial fossa through the pterygoid erosion and inferior orbital fissure. Extension to the anterior portion of the left cavernous sinus is also visible. Black asterisks: sphenoidal inflammatory tissue.
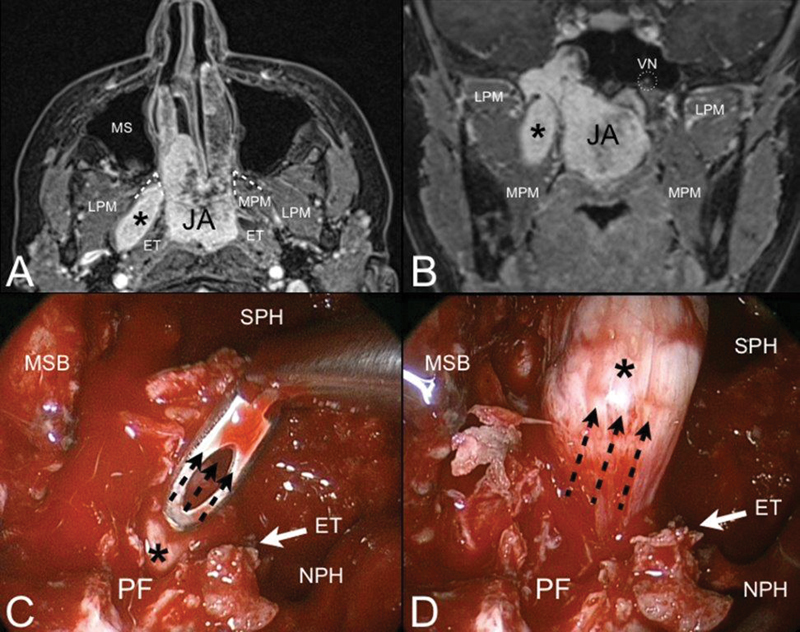
Axial (
A
) and coronal (
B
) contrast-enhanced T1-weighted magnetic resonance (MR). Juvenile angiofibroma (JA) with finger-like retropterygoid extension (black asterisk). Through the bone of the pterygoid root, JA extents to the pterygoid fossa (PF) and follows the direction of the medial pterygoid muscle (MPM) staying behind the auditory tube (ET). Endoscopic view of the right nasal fossa during the endoscopic procedure (
C, D
). The transpterygoid approach allows to expose the pterygoid fossa and pull up (black dashed arrows) the retropterygoid extension of the lesion. Abbreviations: LPM, lateral pterygoid muscle; MS, maxillary sinus; MSB, middle skull base; NPH, nasopharynx; SPH, sphenoid sinus; VN, vidian nerve.
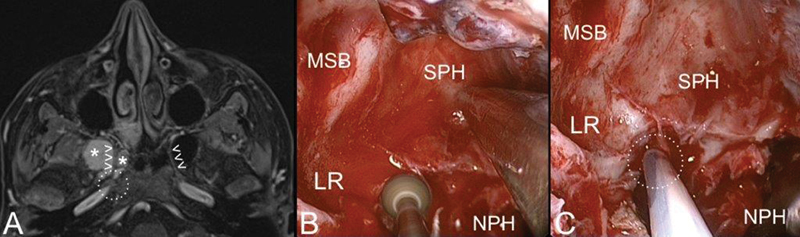
Axial contrast-enhanced T1-weighted magnetic resonance (MR) (
A
) and endoscopic view (
B, C
) of juvenile angiofibroma (white asterisks) extending along the right vidian canal (white arrowheads). After removal of the vidian portion of the lesion, the endoscopic procedure is completed by extensive drilling of the pterygoid root (
B
) till the foramen lacerum (
C
; dashed white circle). Abbreviations: LR, lateral recess; MSB, middle skull base; NPH, nasopharynx; SPH, sphenoid sinus.
References
-
- Lund V J, Stammberger H, Nicolai P et al.European position paper on endoscopic management of tumours of the nose, paranasal sinuses and skull base. Rhinol Suppl. 2010;22:1–143. - PubMed
-
- Antonelli A R, Cappiello J, Di Lorenzo D, Donajo C A, Nicolai P, Orlandini A. Diagnosis, staging, and treatment of juvenile nasopharyngeal angiofibroma (JNA) Laryngoscope. 1987;97(11):1319–1325. - PubMed
-
- Zanation A M, Mitchell C A, Rose A S.Endoscopic skull base techniques for juvenile nasopharyngeal angiofibroma Otolaryngol Clin North Am 20124503711–730., ix ix . - PubMed
-
- Danesi G, Panciera D T, Harvey R J, Agostinis C. Juvenile nasopharyngeal angiofibroma: evaluation and surgical management of advanced disease. Otolaryngol Head Neck Surg. 2008;138(05):581–586. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
