

Advances in Diagnosis and Management of Hemodynamic Instability in Neonatal Shock
- PMID: 29404312
- PMCID: PMC5780410
- DOI: 10.3389/fped.2018.00002
Advances in Diagnosis and Management of Hemodynamic Instability in Neonatal Shock
Abstract
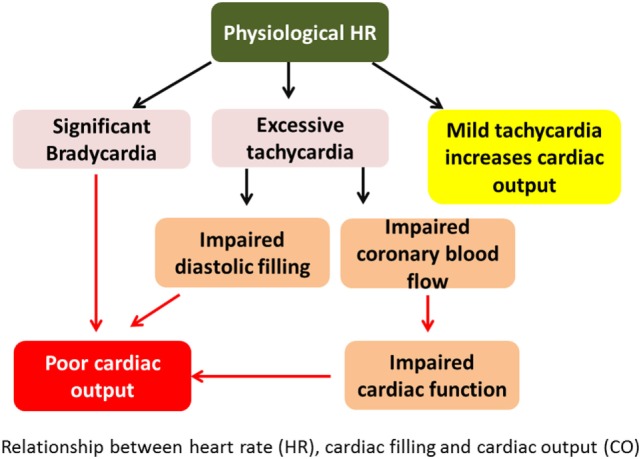
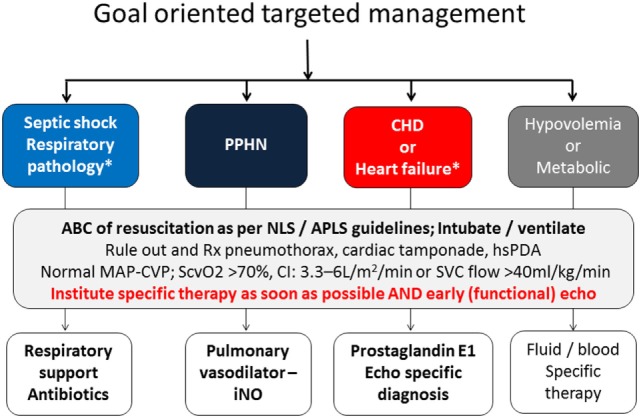
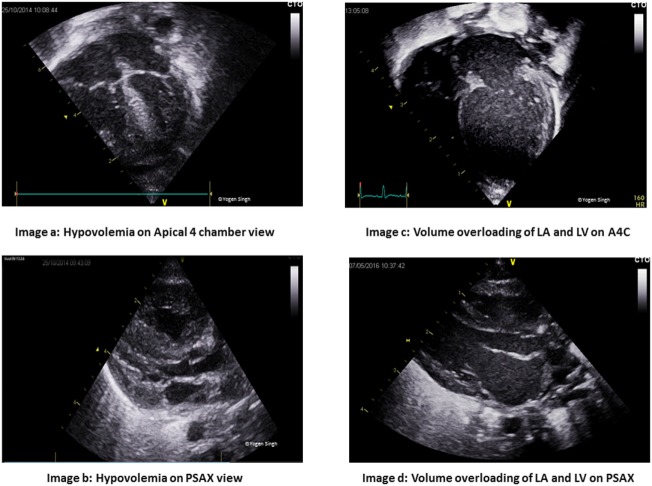
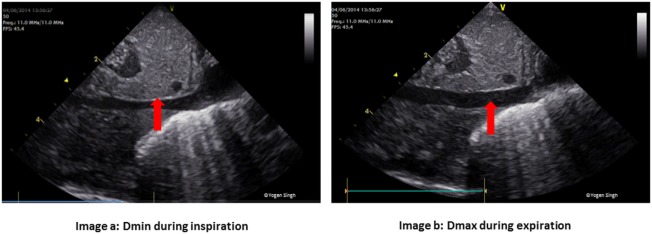
Shock in newborn infants has unique etiopathologic origins that require careful assessment to direct specific interventions. Early diagnosis is key to successful management. Unlike adults and pediatric patients, shock in newborn infants is often recognized in the uncompensated phase by the presence of hypotension, which may be too late. The routine methods of evaluation used in the adult and pediatric population are often invasive and less feasible. We aim to discuss the pathophysiology in shock in newborn infants, including the transitional changes at birth and unique features that contribute to the challenges in early identification. Special emphasis has been placed on bedside focused echocardiography/focused cardiac ultrasound, which can be used as an additional tool for early, neonatologist driven, ongoing evaluation and management. An approach to goal oriented management of shock has been described and how bed side functional echocardiography can help in making a logical choice of intervention (fluid therapy, inotropic therapy or vasopressor therapy) in infants with shock.
Keywords: cardiac output; functional echocardiography; hemodynamic; neonatal shock; tissue perfusion.
Figures

Comment in
-
Commentary: Advances in Diagnosis and Management of Hemodynamic Instability in Neonatal Shock.Front Pediatr. 2018 Mar 26;6:70. doi: 10.3389/fped.2018.00070. eCollection 2018. Front Pediatr. 2018. PMID: 29634044 Free PMC article. No abstract available.
References
-
- Brierley J, Carcillo JA, Choong K, Cornell T, Decaen A, Deymann A, et al. Clinical practice parameters for hemodynamic support of pediatric and neonatal septic shock: 2007 update from the American College of Critical Care Medicine. Crit Care Med (2009) 37:666–88. 10.1097/CCM.0b013e31819323c6 - DOI - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources