

Acute decompensation boosts hepatic collagen type III deposition and deteriorates experimental and human cirrhosis
- PMID: 29404528
- PMCID: PMC5796334
- DOI: 10.1002/hep4.1135
Acute decompensation boosts hepatic collagen type III deposition and deteriorates experimental and human cirrhosis
Abstract
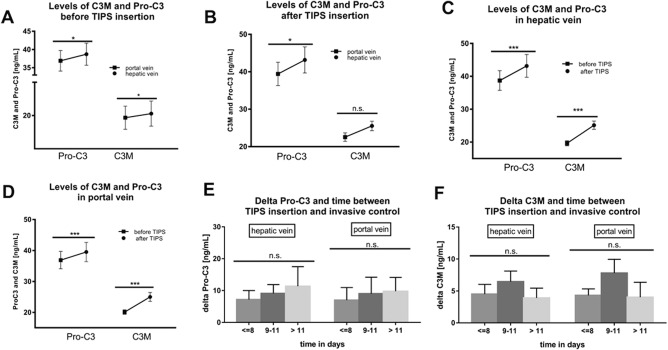
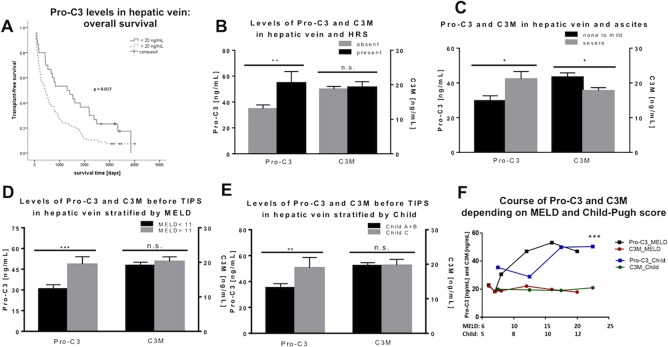
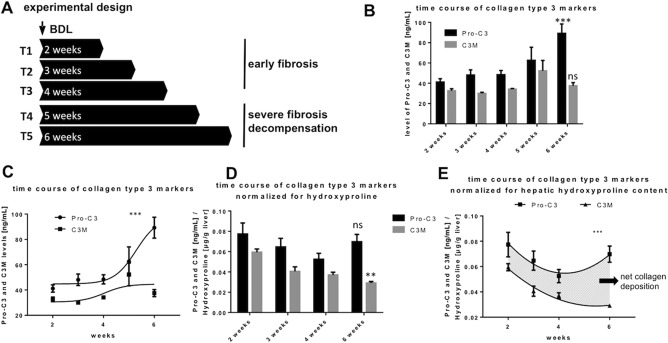
Patients with end-stage liver disease develop acute decompensation (AD) episodes, which become more frequent and might develop into acute-on-chronic liver failure (ACLF). However, it remains unknown how AD induces acceleration of liver disease. We hypothesized that remodeling of collagen type III plays a role in the acceleration of liver cirrhosis after AD and analyzed its formation (Pro-C3) and degradation (matrix metalloproteinase-degraded type III collagen [C3M]) markers in animal models and human disease. Bile duct ligation induced different stages of liver fibrosis in rats. Fibrosis development (hydroxyprolin content, sirius red staining, α-smooth muscle actin immunohistochemistry, messenger RNA of profibrotic cytokines), necroinflammation (aminotransferases levels), fibrolysis (matrix metalloproteinase 2 expression and activity, C1M, C4M), and Pro-C3 and C3M were analyzed 2, 3, 4, 5, and 6 weeks after bile duct ligation (n = 5 each group). In 110 patients with decompensated liver cirrhosis who underwent a transjugular intrahepatic portosystemic shunt procedure for AD, clinical and laboratory parameters as well as Pro-C3 and C3M were measured in blood samples from portal and hepatic veins and were collected just before the transjugular intrahepatic portosystemic shunt placement and 1-3 weeks later. Animal studies showed increased markers of collagen type III deposition with fibrosis, necroinflammation, and decompensation of liver cirrhosis, defined as ascites development. Higher Pro-C3 levels were associated with injury, disease severity scores (Model for End-Stage Liver Disease, Child-Pugh, chronic liver failure-C AD), ACLF development, and mortality. C3M decreased with AD and the chronic liver failure-C AD score. Collagen type III deposition ratio increased with the risk of ACLF development and mortality. Conclusion: We show for the first time that AD boosts collagen type III deposition in experimental and human cirrhosis, possibly contributing to the worsened outcome in patients with decompensated cirrhosis. (Hepatology Communications 2018;2:211-222).
Figures

References
-
- Chirapongsathorn S, Talwalkar JA, Kamath PS. Readmission in cirrhosis: a growing problem. Curr Treat Options Gastroenterol 2016;14:236‐246. - PubMed
-
- Leeming DJ, Anadol E, Schierwagen R, Karsdal MA, Byrjalsen I, Nielsen MJ, et al. Combined antiretroviral therapy attenuates hepatic extracellular matrix remodeling in HIV patients assessed by novel protein fingerprint markers. AIDS 2014. 10;28:2081‐2090. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
