

Downward Trend in Pediatric Resident Laryngoscopy Participation in PICUs
- PMID: 29406378
- PMCID: PMC5935530
- DOI: 10.1097/PCC.0000000000001470
Downward Trend in Pediatric Resident Laryngoscopy Participation in PICUs
Erratum in
-
Downward Trend in Pediatric Resident Laryngoscopy Participation in PICUs: Erratum.Pediatr Crit Care Med. 2020 Jan;21(1):112. doi: 10.1097/PCC.0000000000002199. Pediatr Crit Care Med. 2020. PMID: 31899761 No abstract available.
Abstract
Objectives: As of July 2013, pediatric resident trainee guidelines in the United States no longer require proficiency in nonneonatal tracheal intubation. We hypothesized that laryngoscopy by pediatric residents has decreased over time, with a more pronounced decrease after this guideline change.
Design: Prospective cohort study.
Setting: Twenty-five PICUs at various children's hospitals across the United States.
Patients: Tracheal intubations performed in PICUs from July 2010 to June 2016 in the multicenter tracheal intubation database (National Emergency Airway Registry for Children).
Intervention: None.
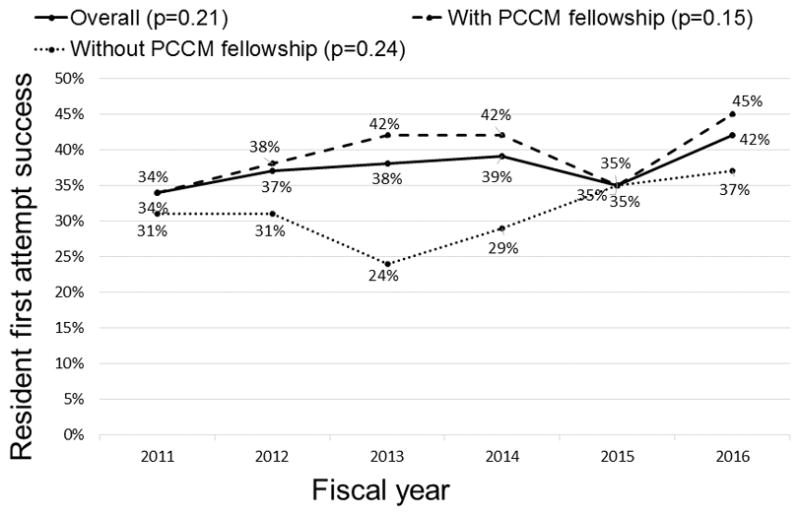
Measurements and main results: Prospective cohort study in which all primary tracheal intubations occurring in the United States from July 2010 to June 2016 in the multicenter tracheal intubation database (National Emergency Airway Registry for Children) were analyzed. Participating PICU leaders were also asked to describe their local airway management training for residents. Resident participation trends over time, stratified by presence of a Pediatric Critical Care Medicine fellowship and airway training curriculum for residents, were described. A total of 9,203 tracheal intubations from 25 PICUs were reported. Pediatric residents participated in 16% of tracheal intubations as first laryngoscopists: 14% in PICUs with a Pediatric Critical Care Medicine fellowship and 34% in PICUs without one (p < 0.001). Resident participation decreased significantly over time (3.4% per year; p < 0.001). The decrease was significant in ICUs with a Pediatric Critical Care Medicine fellowship (p < 0.001) but not in ICUs without one (p = 0.73). After adjusting for site-level clustering, patient characteristics, and Pediatric Critical Care Medicine fellowship presence, the Accreditation Council for Graduate Medical Education guideline change was not associated with lower participation by residents (odds ratio, 0.86; 95% CI, 0.59-1.24; p = 0.43). The downward trend of resident participation was similar regardless of the presence of an airway curriculum for residents.
Conclusion: Laryngoscopy by pediatric residents has substantially decreased over time. This downward trend was not associated with the 2013 Accreditation Council for Graduate Medical Education change in residency requirements.
Trial registration: ClinicalTrials.gov NCT02493478.
Conflict of interest statement
The rest of authors have no conflicts of interest relevant to this article to disclose.
Figures



References
-
- Nishisaki A, Turner DA, Brown CA, et al. A National Emergency Airway Registry for children: landscape of tracheal intubation in 15 PICUs. Crit Care Med. 2013;41(3):874–85. - PubMed
-
- Sanders RC, Giuliano JS, Sullivan JE, et al. Level of trainee and tracheal intubation outcomes. Pediatrics. 2013;131(3):e821–8. - PubMed
-
- Nishisaki A, Donoghue AJ, Colborn S, et al. Effect of just-in-time simulation training on tracheal intubation procedure safety in the pediatric intensive care unit. Anesthesiology. 2010;113(1):214–23. - PubMed
-
- ACGME (Accreditation Council for Graduate Medical Education) [Accessed October 11, 2016];Program Requirements for Graduate Medical Education in Pediatrics. Available at: https://www.acgme.org/Portals/0/PFAssets/ProgramRequirements/320_pediatr....; ACGME approved: September 30, 2012; effective: July 1, 2013. Revised and effective: July 1, 2015. Revised and effective: July 1, 2016.
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
