

Pathophysiological Response to Burn Injury in Adults
- PMID: 29408836
- PMCID: PMC8966302
- DOI: 10.1097/SLA.0000000000002097
Pathophysiological Response to Burn Injury in Adults
Abstract
Objective: The aim of this study was to compare the hypermetabolic, and inflammatory trajectories in burned adults to gain insight into the pathophysiological alterations and outcomes after injury.
Summary of background data: Burn injury leads to a complex response that is associated with hypermetabolism, morbidity, and mortality. The underlying pathophysiology and the correlations between humoral changes and organ function have not been well delineated in adult burn patients.
Methods: Burned adult patients (n = 1288) admitted to our center from 2006 to 2016 were enrolled in this prospective study. Demographics, clinical data, metabolic and inflammatory markers, hypermetabolism, organ function, and clinical outcomes were obtained throughout acute hospitalization. We then stratified patients according to burn size (<20%, 20% to 40%, and >40% total body surface area [TBSA]) and compared biomedical profiles and clinical outcomes for these patients.
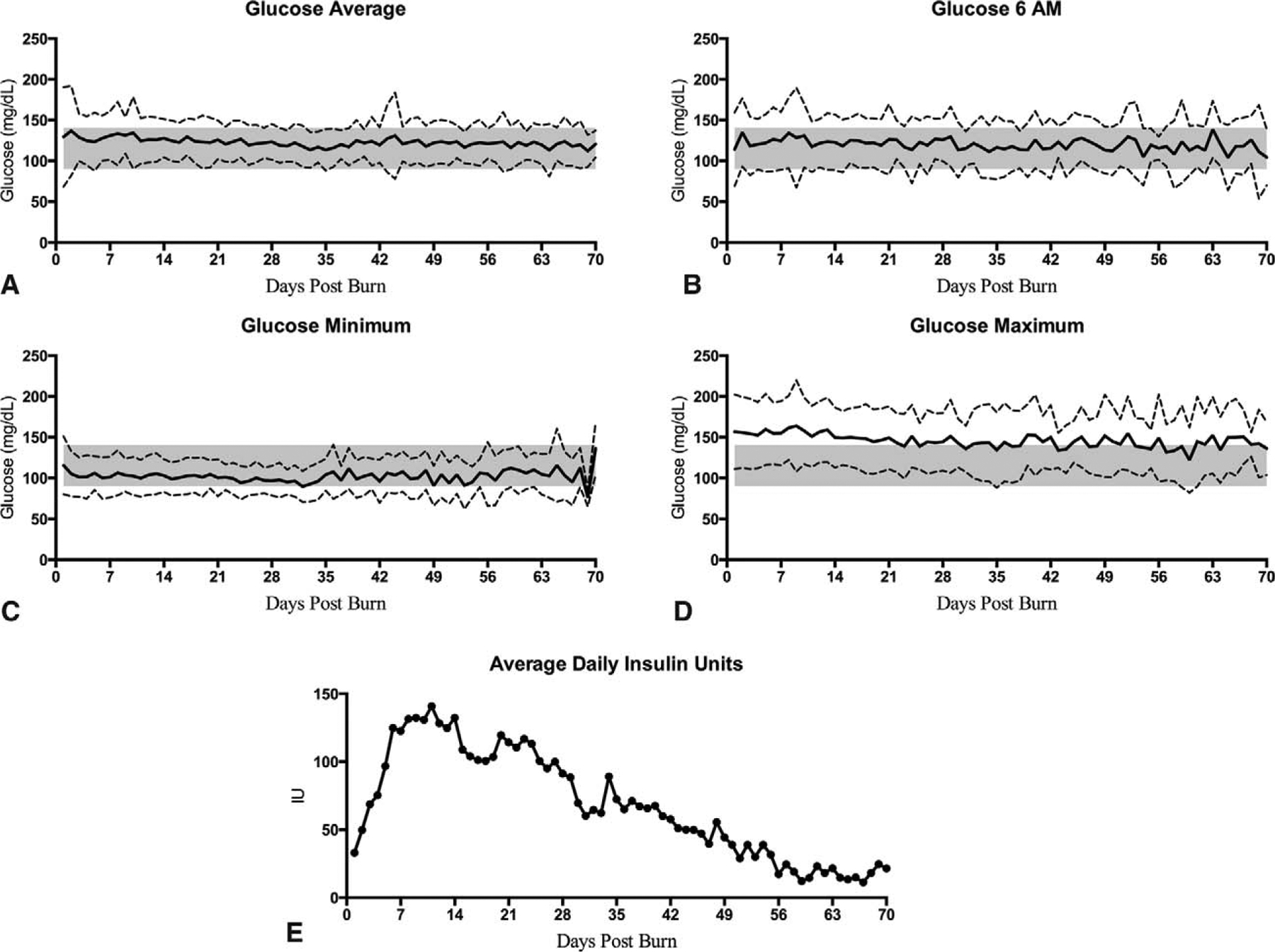
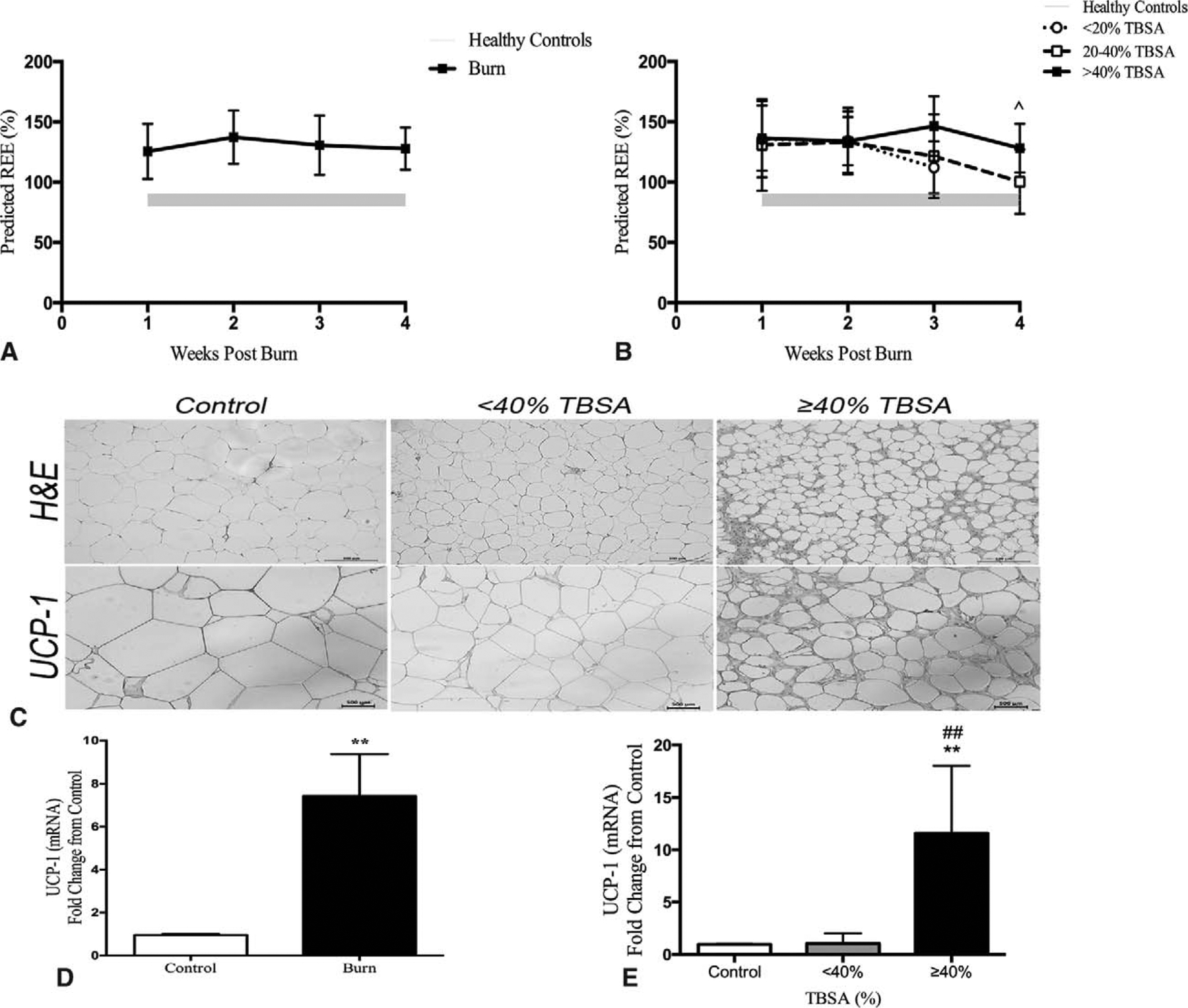
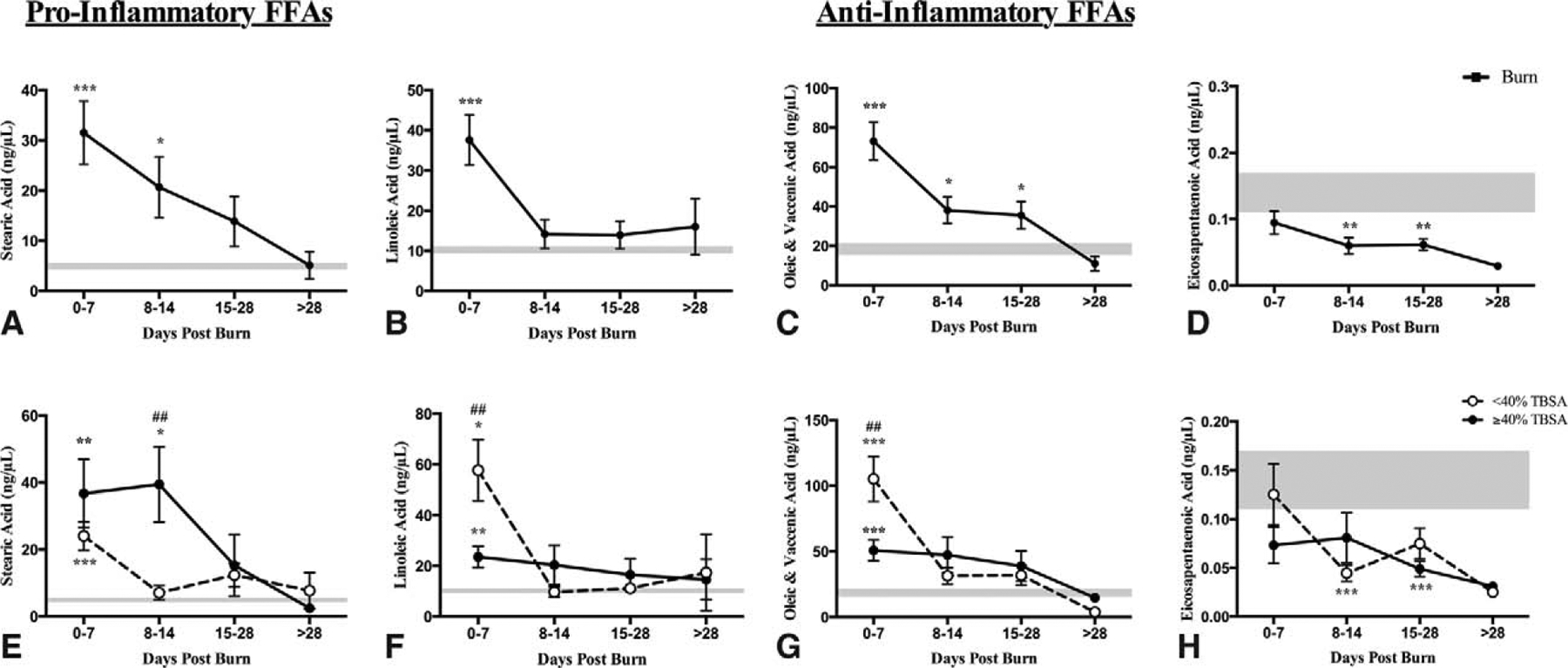
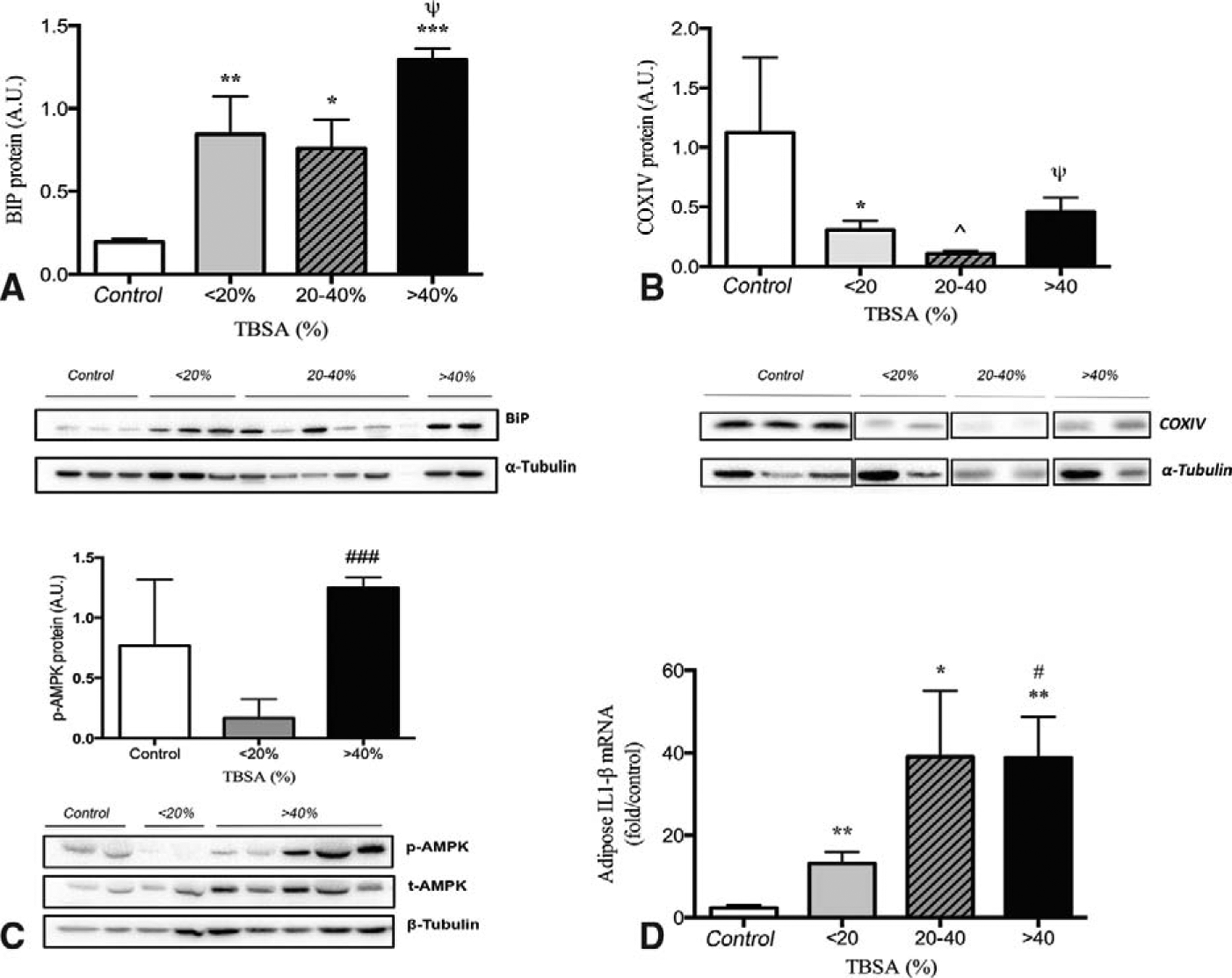
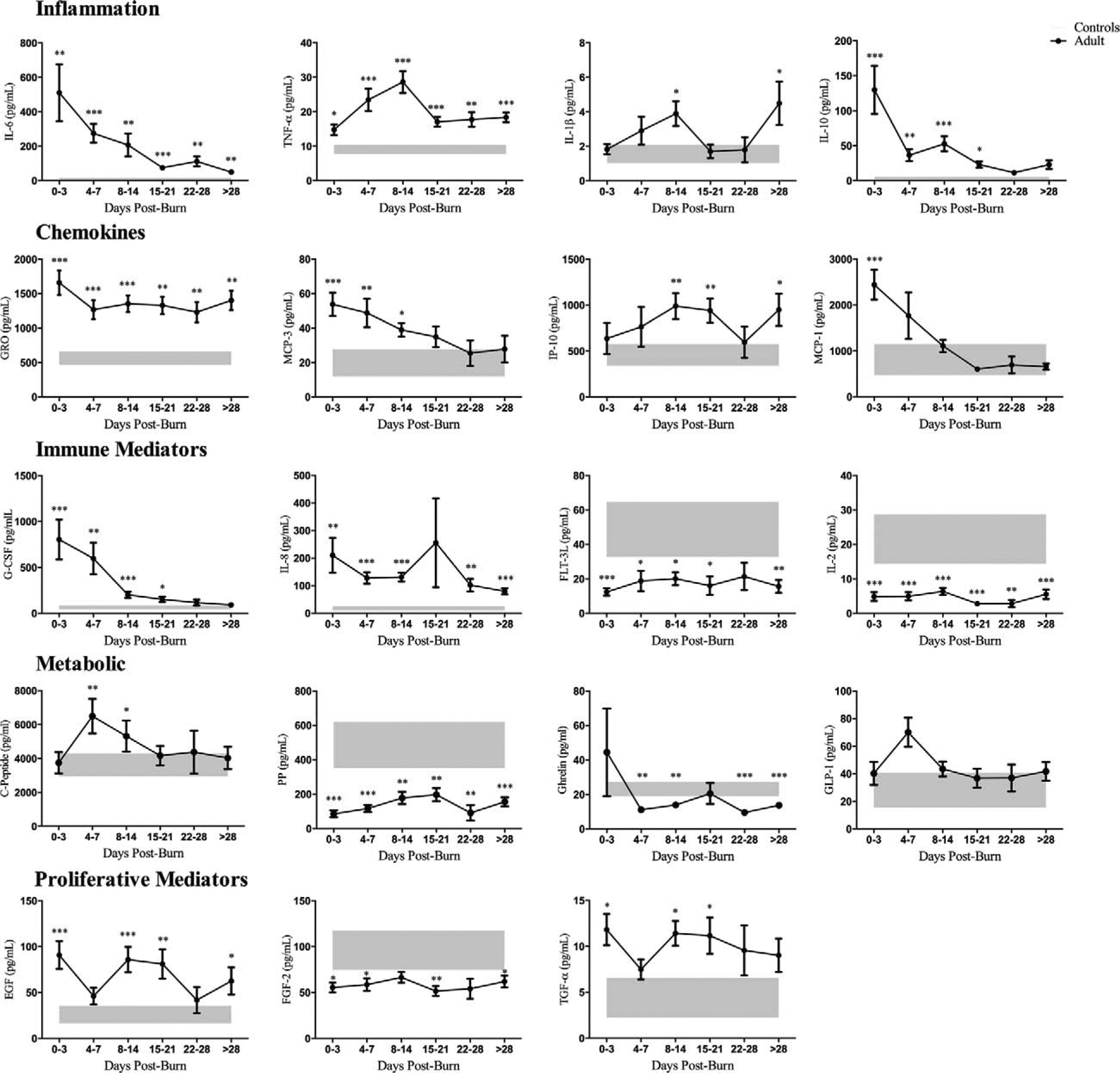
Results: Burn patients were hypermetabolic with elevated resting energy expenditure (REE) associated with increased browning of white adipose tissue from weeks 2 to 4. Hyperglycemia and hyperinsulinemia peaked 7 to 14 days after injury. Oral glucose tolerance and insulin resistance (QUICKI, HOMA2) tests further confirmed these findings with similar areas under the curve for moderate (20% to 40% TBSA) and severe burn (>40% TBSA). Lipid metabolism in sera revealed elevated pro-inflammatory stearic and linoleic acid, with complementary increases in anti-inflammatory free fatty acids. Similar increases were observed for inflammatory cytokines, chemokines, and metabolic hormones. White adipose tissue from the site of injury had increased ER stress, mitochondrial damage, and inflammasome activity, which was exacerbated with increasing burn severity.
Conclusions: In this large prospective trial, we delineated the complexity of the pathophysiologic responses postburn in adults and concluded that these profound responses are time and burn size dependent. Patients with medium-size (20% to 40% TBSA) burn demonstrated a very robust response that is similar to large burns.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
