

Computed tomography in adult patients with primary ciliary dyskinesia: Typical imaging findings
- PMID: 29408869
- PMCID: PMC5800555
- DOI: 10.1371/journal.pone.0191457
Computed tomography in adult patients with primary ciliary dyskinesia: Typical imaging findings
Abstract
Objectives: Among patients with non-cystic fibrosis bronchiectasis, 1-18% have an underlying diagnosis of primary ciliary dyskinesia (PCD) and it is suspected that there is under-recognition of this disease. Our intention was to evaluate the specific features of PCD seen on computed tomography (CT) in the cohort of bronchiectasis in order to facilitate the diagnosis.
Materials and methods: One hundred and twenty-one CTs performed in patients with bronchiectasis were scored for the involvement, type, and lobar distribution of bronchiectasis, bronchial dilatation, and bronchial wall thickening. Later, associated findings such as mucus plugging, tree in bud, consolidations, ground glass opacities, interlobular thickening, intralobular lines, situs inversus, emphysema, mosaic attenuation, and atelectasis were registered. Patients with PCD (n = 46) were compared to patients with other underlying diseases (n = 75).
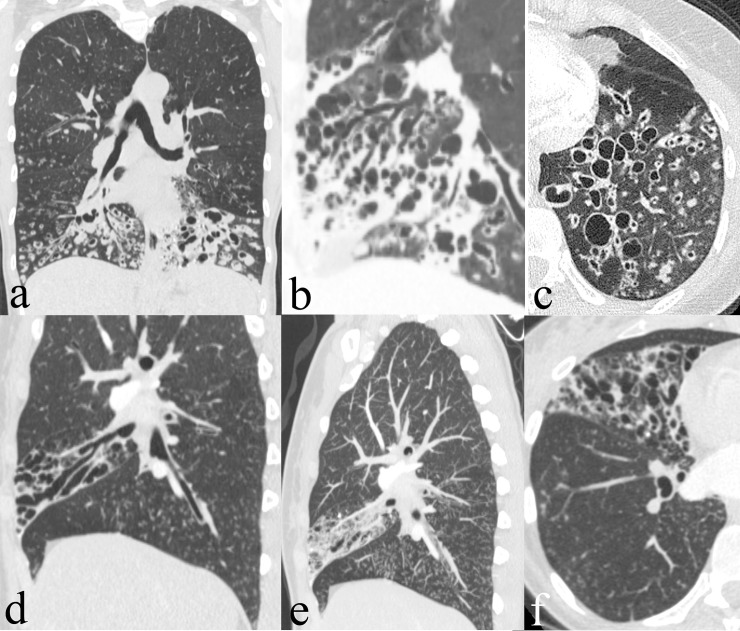
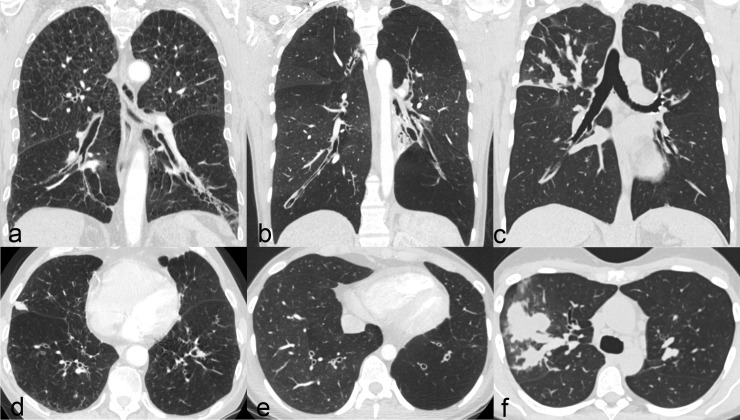
Results: In patients with PCD, the extent and severity of the bronchiectasis and bronchial wall thickness were significantly lower in the upper lung lobes (p<0.001-p = 0.011). The lobar distribution differed significantly with a predominance in the middle and lower lobes in patients with PCD (<0.001). Significantly more common in patients with PCD were mucous plugging (p = 0.001), tree in bud (p <0.001), atelectasis (p = 0.009), and a history of resection of a middle or lower lobe (p = 0.047). Less common were emphysematous (p = 0.003) and fibrotic (p<0.001) changes. A situs inversus (Kartagener's Syndrome) was only seen in patients with PCD (17%, p <0.001).
Conclusion: Typical imaging features in PCD include a predominance of bronchiectasis in the middle and lower lobes, severe tree in bud pattern, mucous plugging, and atelectasis. These findings may help practitioners to identify patients with bronchiectasis in whom further work-up for PCD is called for.
Conflict of interest statement
Figures
References
-
- Barker AF. Bronchiectasis. N Engl J Med. 2002;346: 1383–1393. doi: 10.1056/NEJMra012519 - DOI - PubMed
-
- Lonni S, Chalmers JD, Goeminne PC, McDonnell MJ, Dimakou K, De Soyza A, et al. Etiology of Non-Cystic Fibrosis Bronchiectasis in Adults and Its Correlation to Disease Severity. Ann Am Thorac Soc. 2015;12: 1764–1770. doi: 10.1513/AnnalsATS.201507-472OC - DOI - PMC - PubMed
-
- Lucas JS, Burgess A, Mitchison HM, Moya E, Williamson M, Hogg C, et al. Diagnosis and management of primary ciliary dyskinesia. Arch Dis Child. 2014;99: 850–856. doi: 10.1136/archdischild-2013-304831 - DOI - PMC - PubMed
-
- Milliron B, Henry TS, Veeraraghavan S, Little BP. Bronchiectasis: Mechanisms and Imaging Clues of Associated Common and Uncommon Diseases. Radiogr Rev Publ Radiol Soc N Am Inc. 2015;35: 1011–1030. doi: 10.1148/rg.2015140214 - DOI - PubMed
-
- Altenburg J, Wortel K, van der Werf TS, Boersma WG. Non-cystic fibrosis bronchiectasis: clinical presentation, diagnosis and treatment, illustrated by data from a Dutch Teaching Hospital. Neth J Med. 2015;73: 147–154. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
