

Impact of person-centred care training and person-centred activities on quality of life, agitation, and antipsychotic use in people with dementia living in nursing homes: A cluster-randomised controlled trial
- PMID: 29408901
- PMCID: PMC5800565
- DOI: 10.1371/journal.pmed.1002500
Impact of person-centred care training and person-centred activities on quality of life, agitation, and antipsychotic use in people with dementia living in nursing homes: A cluster-randomised controlled trial
Abstract
Background: Agitation is a common, challenging symptom affecting large numbers of people with dementia and impacting on quality of life (QoL). There is an urgent need for evidence-based, cost-effective psychosocial interventions to improve these outcomes, particularly in the absence of safe, effective pharmacological therapies. This study aimed to evaluate the efficacy of a person-centred care and psychosocial intervention incorporating an antipsychotic review, WHELD, on QoL, agitation, and antipsychotic use in people with dementia living in nursing homes, and to determine its cost.
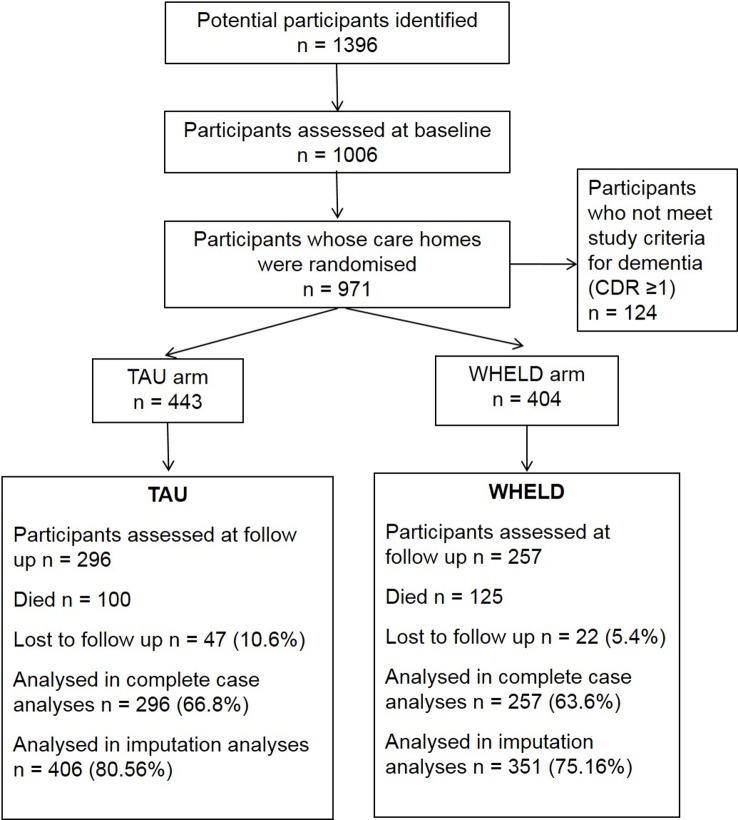
Methods and findings: This was a randomised controlled cluster trial conducted between 1 January 2013 and 30 September 2015 that compared the WHELD intervention with treatment as usual (TAU) in people with dementia living in 69 UK nursing homes, using an intention to treat analysis. All nursing homes allocated to the intervention received staff training in person-centred care and social interaction and education regarding antipsychotic medications (antipsychotic review), followed by ongoing delivery through a care staff champion model. The primary outcome measure was QoL (DEMQOL-Proxy). Secondary outcomes were agitation (Cohen-Mansfield Agitation Inventory [CMAI]), neuropsychiatric symptoms (Neuropsychiatric Inventory-Nursing Home Version [NPI-NH]), antipsychotic use, global deterioration (Clinical Dementia Rating), mood (Cornell Scale for Depression in Dementia), unmet needs (Camberwell Assessment of Need for the Elderly), mortality, quality of interactions (Quality of Interactions Scale [QUIS]), pain (Abbey Pain Scale), and cost. Costs were calculated using cost function figures compared with usual costs. In all, 847 people were randomised to WHELD or TAU, of whom 553 completed the 9-month randomised controlled trial. The intervention conferred a statistically significant improvement in QoL (DEMQOL-Proxy Z score 2.82, p = 0.0042; mean difference 2.54, SEM 0.88; 95% CI 0.81, 4.28; Cohen's D effect size 0.24). There were also statistically significant benefits in agitation (CMAI Z score 2.68, p = 0.0076; mean difference 4.27, SEM 1.59; 95% CI -7.39, -1.15; Cohen's D 0.23) and overall neuropsychiatric symptoms (NPI-NH Z score 3.52, p < 0.001; mean difference 4.55, SEM 1.28; 95% CI -7.07,-2.02; Cohen's D 0.30). Benefits were greatest in people with moderately severe dementia. There was a statistically significant benefit in positive care interactions as measured by QUIS (19.7% increase, SEM 8.94; 95% CI 2.12, 37.16, p = 0.03; Cohen's D 0.55). There were no statistically significant differences between WHELD and TAU for the other outcomes. A sensitivity analysis using a pre-specified imputation model confirmed statistically significant benefits in DEMQOL-Proxy, CMAI, and NPI-NH outcomes with the WHELD intervention. Antipsychotic drug use was at a low stable level in both treatment groups, and the intervention did not reduce use. The WHELD intervention reduced cost compared to TAU, and the benefits achieved were therefore associated with a cost saving. The main limitation was that antipsychotic review was based on augmenting processes within care homes to trigger medical review and did not in this study involve proactive primary care education. An additional limitation was the inherent challenge of assessing QoL in this patient group.
Conclusions: These findings suggest that the WHELD intervention confers benefits in terms of QoL, agitation, and neuropsychiatric symptoms, albeit with relatively small effect sizes, as well as cost saving in a model that can readily be implemented in nursing homes. Future work should consider how to facilitate sustainability of the intervention in this setting.
Trial registration: ISRCTN Registry ISRCTN62237498.
Conflict of interest statement
I have read the journal's policy and the authors of this manuscript have the following competing interest: CB reports grants and personal fees from Acadia pharmaceutical company, grants and personal fees from Lundbeck pharmaceutical company, personal fees from Napp pharmaceutical company, personal fees from Roche pharmaceutical company, personal fees from Orion pharmaceutical company, personal fees from Bial pharmaceutical company, personal fees from Bristol Myer Squibb pharmaceutical company, personal fees from Otusaka pharmaceutical company, personal fees from Novartis pharmaceutical company, personal feees from Sunovion, outside the submitted work; AC reports personal fees from Lundbeck, personal fees from Novartis, personal fees from Bial, personal fees from Acadia, personal fees from Sunovion, outside the submitted work; MO, JF, JW, EMC, BW, AC and CB report grants from NIHR, during the conduct of the study. All other authors have nothing to disclose.
Figures
References
-
- Alzheimer’s Disease International. World Alzheimer report 2009. London: Alzheimer’s Disease International; 2009. [cited 2018 Jan 8]. Available from: http://www.alz.co.uk/research/files/WorldAlzheimerReport.pdf.
-
- Alzheimer’s Disease International. World Alzheimer’s report 2013: journey of caring—an analysis of long-term care in dementia. London: Alzheimer’s Disease International; 2013. [cited 2018 Jan 8]. Available from: http://www.alz.co.uk/research/WorldAlzheimerReport2013ExecutiveSummary.pdf.
-
- Ballard C, Corbett A, Howard R. Prescription of antipsychotics in people with dementia. Br J Psychiatry. 2014;205(1):4–5. doi: 10.1192/bjp.bp.113.128710 - DOI - PubMed
-
- Ballard C, Corbett A. Agitation and aggression in people with Alzheimer’s disease. Curr Opin Psychiatry. 2013;26(3):252–9. doi: 10.1097/YCO.0b013e32835f414b - DOI - PubMed
-
- Testad I, Corbett A, Aarsland D, Lexow KO, Fossey J, Woods B, et al. The value of personalized psychosocial interventions to address behavioral and psychological symptoms in people with dementia living in care home settings: a systematic review. Int Psychogeriatr. 2014;26(7):1083–98. doi: 10.1017/S1041610214000131 - DOI - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
