

Malaria Coinfections in Febrile Pediatric Inpatients: A Hospital-Based Study From Ghana
- PMID: 29408951
- PMCID: PMC5982794
- DOI: 10.1093/cid/cix1120
Malaria Coinfections in Febrile Pediatric Inpatients: A Hospital-Based Study From Ghana
Abstract
Background: The epidemiology of pediatric febrile illness is shifting in sub-Saharan Africa, but malaria remains a major cause of childhood morbidity and mortality. The present study describes causes of febrile illness in hospitalized children in Ghana and aims to determine the burden of malaria coinfections and their association with parasite densities.
Methods: In a prospective study, children (aged ≥30 days and ≤15 years) with fever ≥38.0°C were recruited after admission to the pediatric ward of a primary hospital in Ghana. Malaria parasitemia was determined and blood, stool, urine, respiratory, and cerebrospinal fluid specimens were screened for parasitic, bacterial, and viral pathogens. Associations of Plasmodium densities with other pathogens were calculated.
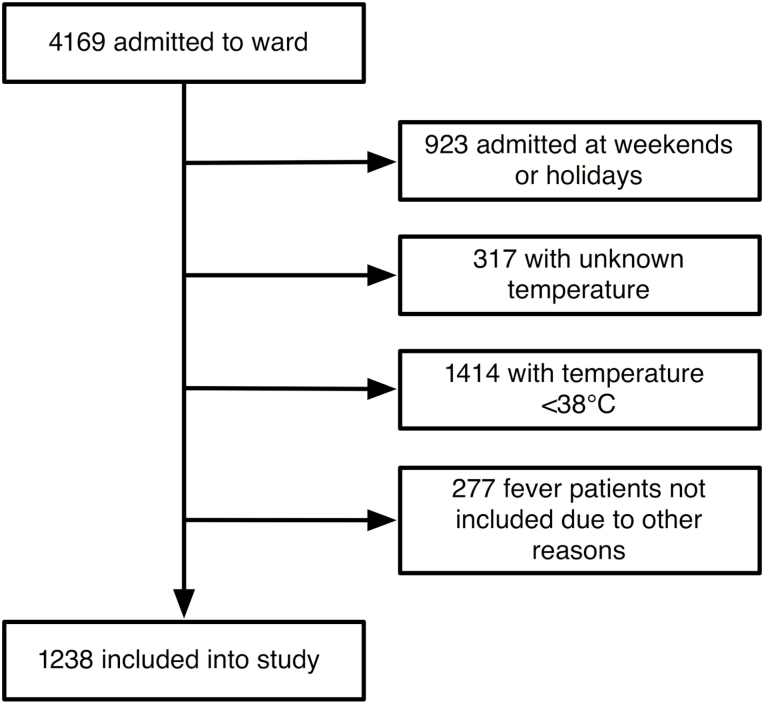
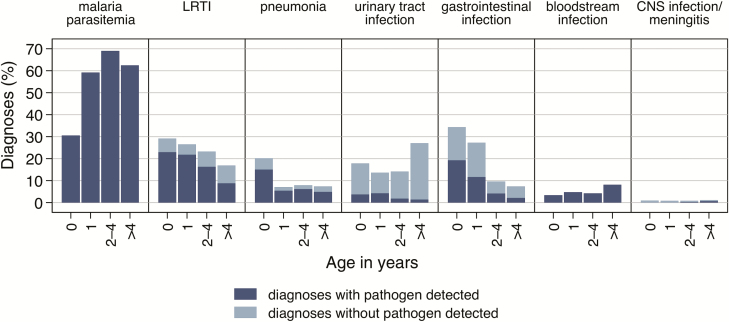
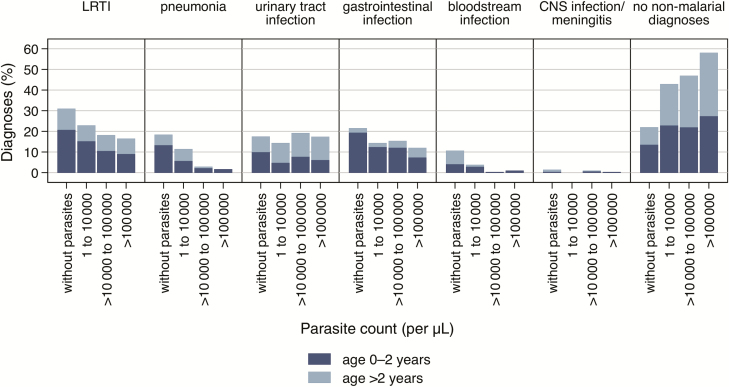
Results: From November 2013 to April 2015, 1238 children were enrolled from 4169 admissions. A clinical/microbiological diagnosis could be made in 1109/1238 (90%) patients, with Plasmodium parasitemia (n = 728/1238 [59%]) being predominant. This was followed by lower respiratory tract infections/pneumonia (n = 411/1238 [34%]; among detected pathogens most frequently Streptococcus pneumoniae, n = 192/299 [64%]), urinary tract infections (n = 218/1238 [18%]; Escherichia coli, n = 21/32 [66%]), gastrointestinal infections (n = 210 [17%]; rotavirus, n = 32/97 [33%]), and invasive bloodstream infections (n = 62 [5%]; Salmonella species, n = 47 [76%]). In Plasmodium-infected children the frequency of lower respiratory tract, gastrointestinal, and bloodstream infections increased with decreasing parasite densities.
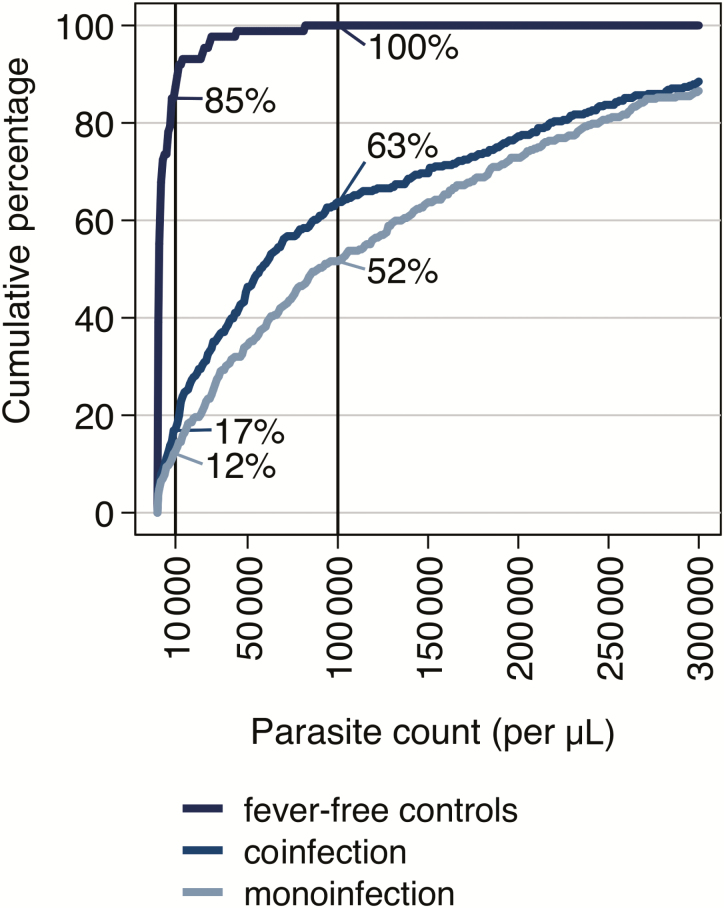
Conclusions: In a hospital setting, the likelihood of comorbidity with a nonmalarial disease is inversely correlated with increasing blood levels of malaria parasites. Hence, parasite densities provide important information as an indicator for the probability of coinfection, in particular to guide antimicrobial medication.
Figures
References
-
- D’Acremont V, Kilowoko M, Kyungu E et al. Beyond malaria—causes of fever in outpatient Tanzanian children. N Engl J Med 2014; 370:809–17. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
