

The characteristics of 76 atypical neurofibromas as precursors to neurofibromatosis 1 associated malignant peripheral nerve sheath tumors
- PMID: 29409029
- PMCID: PMC5961015
- DOI: 10.1093/neuonc/noy013
The characteristics of 76 atypical neurofibromas as precursors to neurofibromatosis 1 associated malignant peripheral nerve sheath tumors
Abstract
Background: Neurofibromatosis 1 (NF1) leads to the development of benign and malignant peripheral nerve sheath tumors (MPNST). MPNST have been described to develop in preexisting benign plexiform neurofibromas (PN) and have a poor prognosis. Atypical neurofibromas (ANF) were recently described as precursor lesions for MPNST, making early detection and management of ANF a possible strategy to prevent MPNST. We aimed to clinically characterize ANF and identify management approaches.
Methods: We analyzed clinical, imaging, and pathology findings of all patients with NF1 and ANF at 3 institutions.
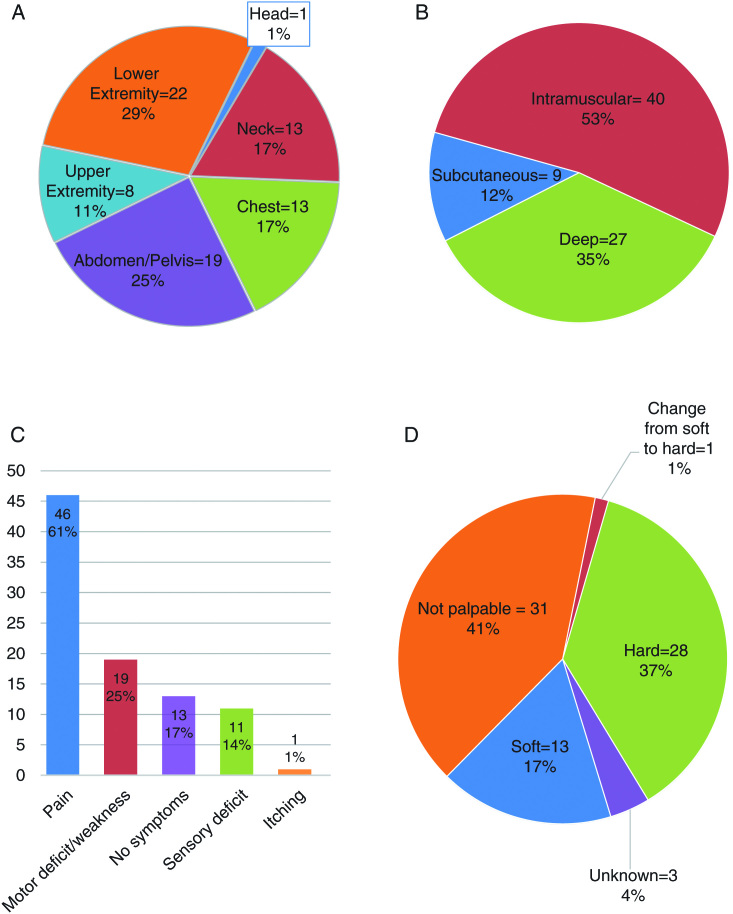
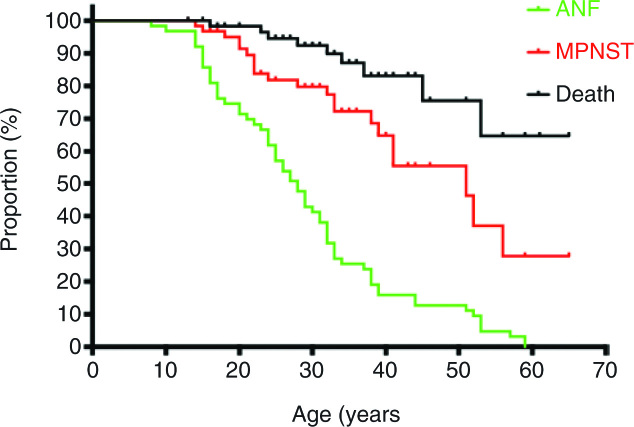
Results: Sixty-three patients had 76 ANF (32M/31F; median age 27.1 y). On MRI, most ANF appeared as distinct nodular lesions and were 18F-fluorodeoxyglucose (FDG) avid. Forty-six ANF were associated with pain, 19 with motor weakness, 45 were palpable or visible, and 13 had no clinical signs. Completely resected ANF (N = 57) have not recurred (median follow-up, 4.1 y; range, 0-14 y). Four ANF transformed into MPNST and 17 patients had a history of MPNST in a different location than was their ANF.
Conclusions: Growth of distinct nodular lesions, pain, and FDG-PET avidity should raise concern for ANF in NF1. Patients with ANF are at greater risk for development of MPNST. Complete resection of ANF may prevent development of MPNST.
Figures
Comment in
-
How should adult patients with neurofibromatosis 1 be managed?Neuro Oncol. 2018 May 18;20(6):721-722. doi: 10.1093/neuonc/noy050. Neuro Oncol. 2018. PMID: 29788480 Free PMC article. No abstract available.
References
-
- Cawthon RM, Weiss R, Xu GF et al. . A major segment of the neurofibromatosis type 1 gene: cDNA sequence, genomic structure, and point mutations. Cell. 1990;62(1):193–201. - PubMed
-
- Martin GA, Viskochil D, Bollag G et al. . The GAP-related domain of the neurofibromatosis type 1 gene product interacts with ras p21. Cell. 1990;63(4):843–849. - PubMed
-
- Wallace MR, Marchuk DA, Andersen LB et al. . Type 1 neurofibromatosis gene: identification of a large transcript disrupted in three NF1 patients. Science. 1990;249(4965):181–186. - PubMed
-
- DeBella K, Szudek J, Friedman JM. Use of the national institutes of health criteria for diagnosis of neurofibromatosis 1 in children. Pediatrics. 2000;105(3 Pt 1):608–614. - PubMed
-
- Friedman JM. Neurofibromatosis 1: clinical manifestations and diagnostic criteria. J Child Neurol. 2002;17(8):548–554; discussion 571–572, 646–651. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
