

A dashboard-based system for supporting diabetes care
- PMID: 29409033
- PMCID: PMC7647008
- DOI: 10.1093/jamia/ocx159
A dashboard-based system for supporting diabetes care
Abstract
Objective: To describe the development, as part of the European Union MOSAIC (Models and Simulation Techniques for Discovering Diabetes Influence Factors) project, of a dashboard-based system for the management of type 2 diabetes and assess its impact on clinical practice.
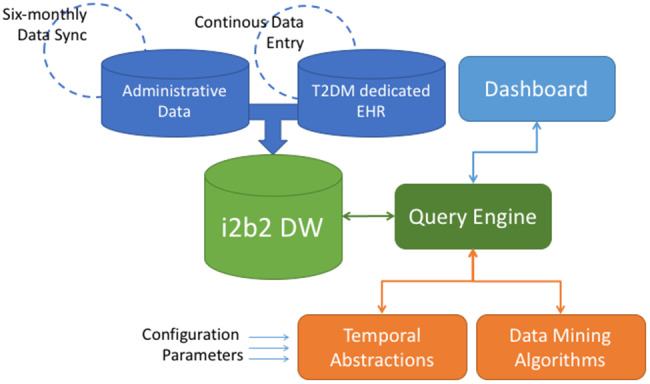
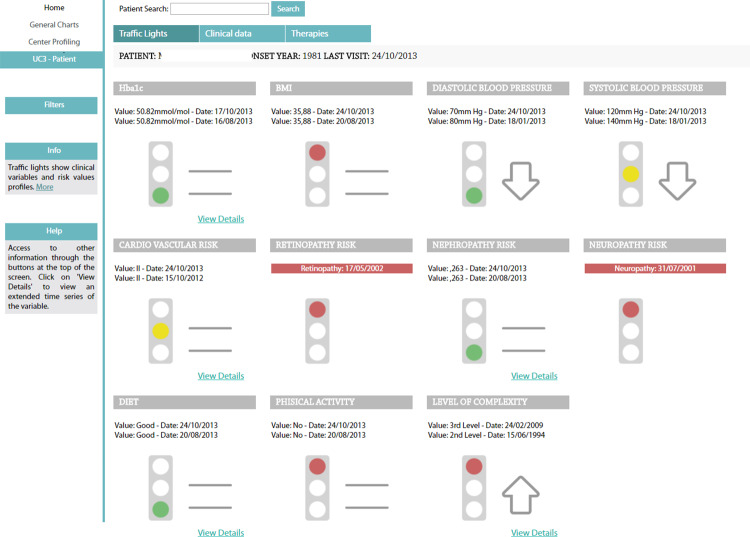
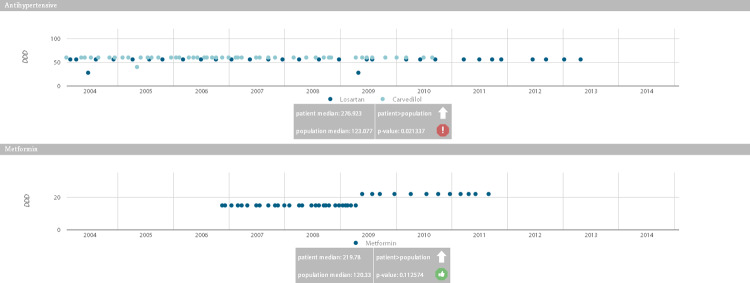
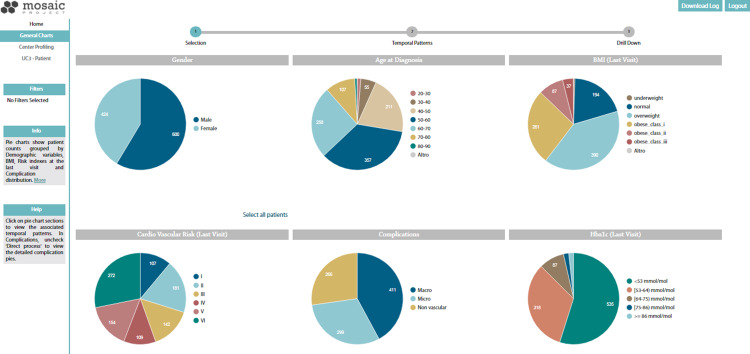
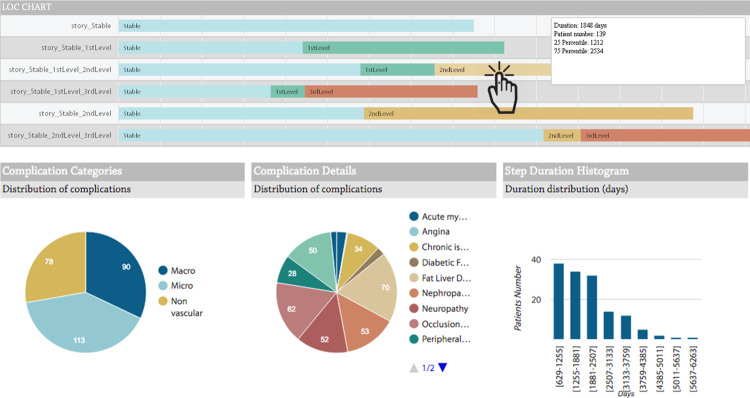
Methods: The MOSAIC dashboard system is based on predictive modeling, longitudinal data analytics, and the reuse and integration of data from hospitals and public health repositories. Data are merged into an i2b2 data warehouse, which feeds a set of advanced temporal analytic models, including temporal abstractions, care-flow mining, drug exposure pattern detection, and risk-prediction models for type 2 diabetes complications. The dashboard has 2 components, designed for (1) clinical decision support during follow-up consultations and (2) outcome assessment on populations of interest. To assess the impact of the clinical decision support component, a pre-post study was conducted considering visit duration, number of screening examinations, and lifestyle interventions. A pilot sample of 700 Italian patients was investigated. Judgments on the outcome assessment component were obtained via focus groups with clinicians and health care managers.
Results: The use of the decision support component in clinical activities produced a reduction in visit duration (P ≪ .01) and an increase in the number of screening exams for complications (P < .01). We also observed a relevant, although nonstatistically significant, increase in the proportion of patients receiving lifestyle interventions (from 69% to 77%). Regarding the outcome assessment component, focus groups highlighted the system's capability of identifying and understanding the characteristics of patient subgroups treated at the center.
Conclusion: Our study demonstrates that decision support tools based on the integration of multiple-source data and visual and predictive analytics do improve the management of a chronic disease such as type 2 diabetes by enacting a successful implementation of the learning health care system cycle.
Figures

References
-
- Palmer AJ, Roze S, Valentine WJ et al. , The CORE Diabetes Model: Projecting long-term clinical outcomes, costs and cost-effectiveness of interventions in diabetes mellitus (types 1 and 2) to support clinical and reimbursement decision-making. Curr Med Res Opin. 2004;20(Suppl 1):S5–26. - PubMed
-
- Donsa K, Beck P, Höll B et al. , Impact of errors in paper-based and computerized diabetes management with decision support for hospitalized patients with type 2 diabetes. A post-hoc analysis of a before and after study. Int J Med Inform. 2016;90:58–67. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
