

Cost-effectiveness of emergency contraception options over 1 year
- PMID: 29409847
- PMCID: PMC6457123
- DOI: 10.1016/j.ajog.2018.01.025
Cost-effectiveness of emergency contraception options over 1 year
Abstract
Background: The copper intrauterine device is the most effective form of emergency contraception and can also provide long-term contraception. The levonorgestrel intrauterine device has also been studied in combination with oral levonorgestrel for women seeking emergency contraception. However, intrauterine devices have higher up-front costs than oral methods, such as ulipristal acetate and levonorgestrel. Health care payers and decision makers (eg, health care insurers, government programs) with financial constraints must determine if the increased effectiveness of intrauterine device emergency contraception methods are worth the additional costs.
Objective: We sought to compare the cost-effectiveness of 4 emergency contraception strategies-ulipristal acetate, oral levonorgestrel, copper intrauterine device, and oral levonorgestrel plus same-day levonorgestrel intrauterine device-over 1 year from a US payer perspective.
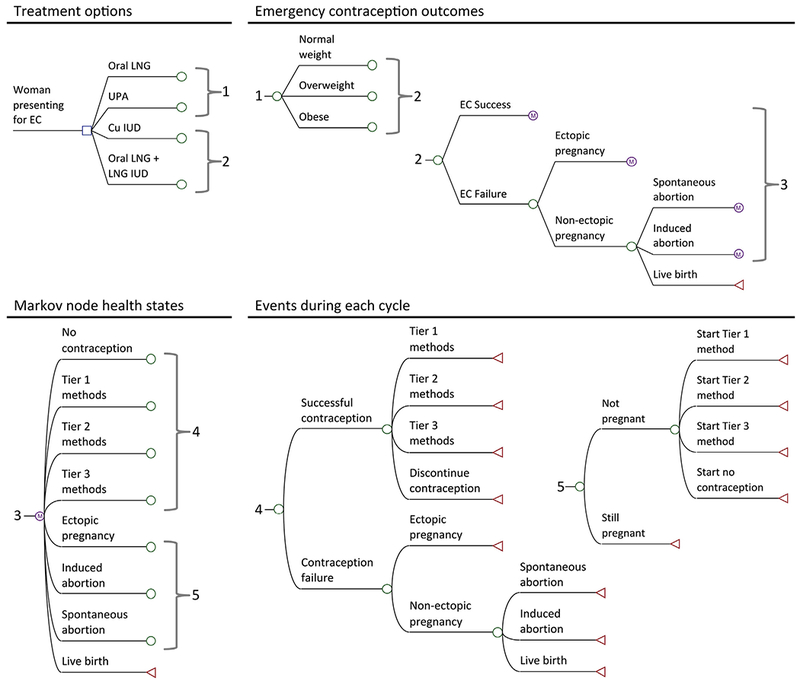
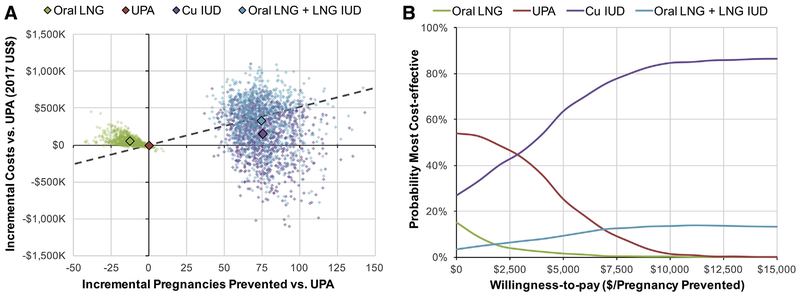
Study design: Costs (2017 US dollars) and pregnancies were estimated over 1 year using a Markov model of 1000 women seeking emergency contraception. Every 28-day cycle, the model estimated the predicted number of pregnancy outcomes (ie, live birth, ectopic pregnancy, spontaneous abortion, or induced abortion) resulting from emergency contraception failure and subsequent contraception use. Model inputs were derived from published literature and national sources. An emergency contraception strategy was considered cost-effective if the incremental cost-effectiveness ratio (ie, the cost to prevent 1 additional pregnancy) was less than the weighted average cost of pregnancy outcomes in the United States ($5167). The incremental cost-effectiveness ratios and probability of being the most cost-effective emergency contraception strategy were calculated from 1000 probabilistic model iterations. One-way sensitivity analyses were used to examine uncertainty in the cost of emergency contraception, subsequent contraception, and pregnancy outcomes as well as the model probabilities.
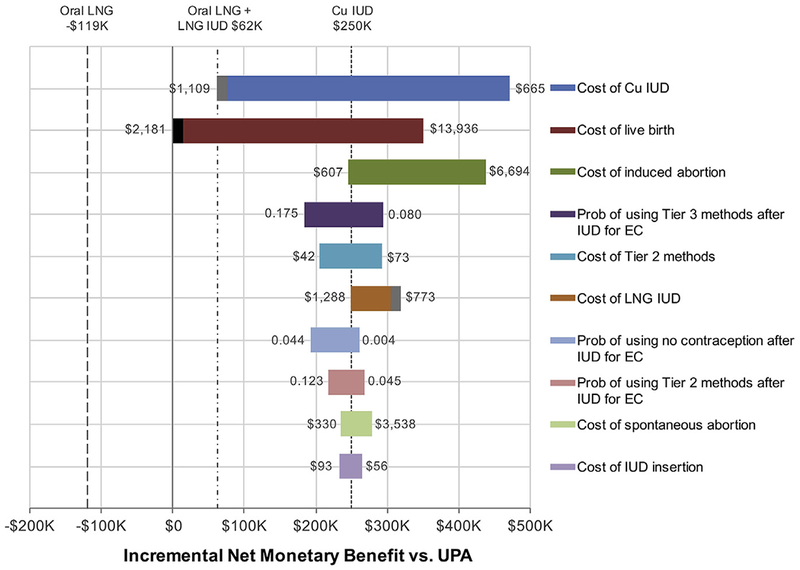
Results: In 1000 women seeking emergency contraception, the model estimated direct medical costs of $1,228,000 and 137 unintended pregnancies with ulipristal acetate, compared to $1,279,000 and 150 unintended pregnancies with oral levonorgestrel, $1,376,000 and 61 unintended pregnancies with copper intrauterine devices, and $1,558,000 and 63 unintended pregnancies with oral levonorgestrel plus same-day levonorgestrel intrauterine device. The copper intrauterine device was the most cost-effective emergency contraception strategy in the majority (63.9%) of model iterations and, compared to ulipristal acetate, cost $1957 per additional pregnancy prevented. Model estimates were most sensitive to changes in the cost of the copper intrauterine device (with higher copper intrauterine device costs, oral levonorgestrel plus same-day levonorgestrel intrauterine device became the most cost-effective option) and the cost of a live birth (with lower-cost births, ulipristal acetate became the most cost-effective option). When the proportion of obese women in the population increased, the copper intrauterine device became even more most cost-effective.
Conclusion: Over 1 year, the copper intrauterine device is currently the most cost-effective emergency contraception option. Policy makers and health care insurance companies should consider the potential for long-term savings when women seeking emergency contraception can promptly obtain whatever contraceptive best meets their personal preferences and needs; this will require removing barriers and promoting access to intrauterine devices at emergency contraception visits.
Keywords: cost-effectiveness analysis; emergency contraception; incremental cost-effectiveness ratio; intrauterine device.
Copyright © 2018 Elsevier Inc. All rights reserved.
Figures
Similar articles
-
Canadian Contraception Consensus (Part 2 of 4).J Obstet Gynaecol Can. 2015 Nov;37(11):1033-9. doi: 10.1016/s1701-2163(16)30054-8. J Obstet Gynaecol Can. 2015. PMID: 26629725 English, French.
-
Canadian Contraception Consensus (Part 1 of 4).J Obstet Gynaecol Can. 2015 Oct;37(10):936-42. doi: 10.1016/s1701-2163(16)30033-0. J Obstet Gynaecol Can. 2015. PMID: 26606712 English, French.
-
Ulipristal acetate compared to levonorgestrel emergency contraception among current oral contraceptive users: a cost-effectiveness analysis.Contraception. 2019 Sep;100(3):222-227. doi: 10.1016/j.contraception.2019.05.004. Epub 2019 May 16. Contraception. 2019. PMID: 31102631
-
The price of emergency contraception in the United States: what is the cost-effectiveness of ulipristal acetate versus single-dose levonorgestrel?Contraception. 2013 Mar;87(3):385-90. doi: 10.1016/j.contraception.2012.08.034. Epub 2012 Oct 4. Contraception. 2013. PMID: 23040122
-
Emergency Contraception.Mayo Clin Proc. 2016 Jun;91(6):802-7. doi: 10.1016/j.mayocp.2016.02.018. Mayo Clin Proc. 2016. PMID: 27261868 Review.
Cited by
-
Emergency contraception subsidy in Canada: a comparative policy analysis.BMC Health Serv Res. 2022 Sep 1;22(1):1110. doi: 10.1186/s12913-022-08416-1. BMC Health Serv Res. 2022. PMID: 36050668 Free PMC article.
-
Effect of Mirena placement on reproductive hormone levels at different time intervals after artificial abortion.World J Clin Cases. 2022 Jan 14;10(2):511-517. doi: 10.12998/wjcc.v10.i2.511. World J Clin Cases. 2022. PMID: 35097076 Free PMC article.
-
Modeling the impact of a health coaching intervention to prevent teen pregnancy.Prev Med Rep. 2022 Jan 29;26:101716. doi: 10.1016/j.pmedr.2022.101716. eCollection 2022 Apr. Prev Med Rep. 2022. PMID: 35169533 Free PMC article.
-
Reversible Contraception in Males: An Obtainable Target?Biology (Basel). 2024 Apr 25;13(5):291. doi: 10.3390/biology13050291. Biology (Basel). 2024. PMID: 38785772 Free PMC article. Review.
References
-
- Belden P, Harper CC, Speidel JJ. The copper IUD for emergency contraception, a neglected option. Contraception 2012;85:338–9. - PubMed
-
- Trussell J The cost of unintended pregnancy in the United States. Contraception 2007;75:168–70. - PubMed
-
- Glasier A, Cameron ST, Blithe D, et al. Can we identify women at risk of pregnancy despite using emergency contraception? Data from randomized trials of ulipristal acetate and levonorgestrel. Contraception 2011;84:363–7. - PubMed
-
- Thomas CM, Schmid R, Cameron S. Is it worth paying more for emergency hormonal contraception? The cost-effectiveness of ulipristal acetate versus levonorgestrel 1.5 mg. J Fam Plann Reprod Health Care 2010;36:197–201. - PubMed
