

Hospital-Level Care at Home for Acutely Ill Adults: a Pilot Randomized Controlled Trial
- PMID: 29411238
- PMCID: PMC5910347
- DOI: 10.1007/s11606-018-4307-z
Hospital-Level Care at Home for Acutely Ill Adults: a Pilot Randomized Controlled Trial
Abstract
Background: Hospitals are standard of care for acute illness, but hospitals can be unsafe, uncomfortable, and expensive. Providing substitutive hospital-level care in a patient's home potentially reduces cost while maintaining or improving quality, safety, and patient experience, although evidence from randomized controlled trials in the US is lacking.
Objective: Determine if home hospital care reduces cost while maintaining quality, safety, and patient experience.
Design: Randomized controlled trial.
Participants: Adults admitted via the emergency department with any infection or exacerbation of heart failure, chronic obstructive pulmonary disease, or asthma.
Intervention: Home hospital care, including nurse and physician home visits, intravenous medications, continuous monitoring, video communication, and point-of-care testing.
Main measures: Primary outcome was direct cost of the acute care episode. Secondary outcomes included utilization, 30-day cost, physical activity, and patient experience.
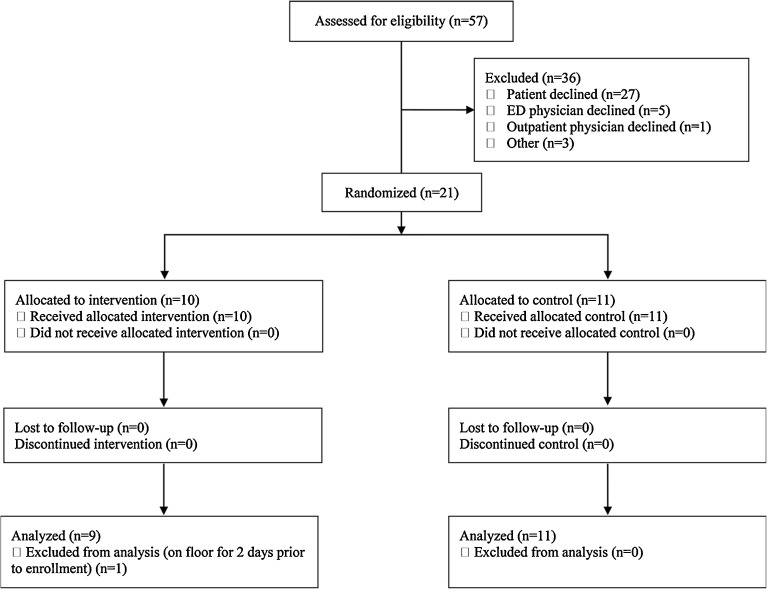
Key results: Nine patients were randomized to home, 11 to usual care. Median direct cost of the acute care episode for home patients was 52% (IQR, 28%; p = 0.05) lower than for control patients. During the care episode, home patients had fewer laboratory orders (median per admission: 6 vs. 19; p < 0.01) and less often received consultations (0% vs. 27%; p = 0.04). Home patients were more physically active (median minutes, 209 vs. 78; p < 0.01), with a trend toward more sleep. No adverse events occurred in home patients, one occurred in control patients. Median direct cost for the acute care plus 30-day post-discharge period for home patients was 67% (IQR, 77%; p < 0.01) lower, with trends toward less use of home-care services (22% vs. 55%; p = 0.08) and fewer readmissions (11% vs. 36%; p = 0.32). Patient experience was similar in both groups.
Conclusions: The use of substitutive home-hospitalization compared to in-hospital usual care reduced cost and utilization and improved physical activity. No significant differences in quality, safety, and patient experience were noted, with more definitive results awaiting a larger trial. Trial Registration NCT02864420.
Keywords: home hospital; home-based care; hospital alternative; hospital at home.
Conflict of interest statement
Prior Presentations
Society of General Internal Medicine—national conference; Washington, DC, 2017. Awarded Lipkin Award.
Conflicts of Interest
The authors declare that they do not have a conflict of interest.
Figures
References
-
- National and State Healthcare-Associated Infections Progress Report. 2016. http://www.cdc.gov/hai/surveillance/progress-report/index.html. Accessed 10 December 2017.
-
- Counsell SR, Holder CM, Liebenauer LL, et al. Effects of a multicomponent intervention on functional outcomes and process of care in hospitalized older patients: a randomized controlled trial of acute care for elders (ACE) in a community hospital. J Am Geriatr Soc. 2000;48(12):1572–1581. doi: 10.1111/j.1532-5415.2000.tb03866.x. - DOI - PubMed
-
- Health, United States, 2015: with special feature on racial and ethnic health disparities. Hyattsville, MD; 2016. https://www.cdc.gov/nchs/data/hus/hus15.pdf. Accessed December 10, 2017. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
