

Socio-economic status and time trends associated with early ART initiation following primary HIV infection in Montreal, Canada: 1996 to 2015
- PMID: 29412520
- PMCID: PMC5804015
- DOI: 10.1002/jia2.25034
Socio-economic status and time trends associated with early ART initiation following primary HIV infection in Montreal, Canada: 1996 to 2015
Abstract
Introduction: Guidelines regarding antiretroviral therapy (ART) initiation in HIV infection have varied over time, with the 2015 World Health Organization recommendation suggesting ART initiation at the time of diagnosis regardless of CD4 T-cell counts. Herein, we investigated the influence of socio-demographic and clinical factors in addition to time trends on early ART initiation among participants of the Montreal Primary HIV Infection Study.
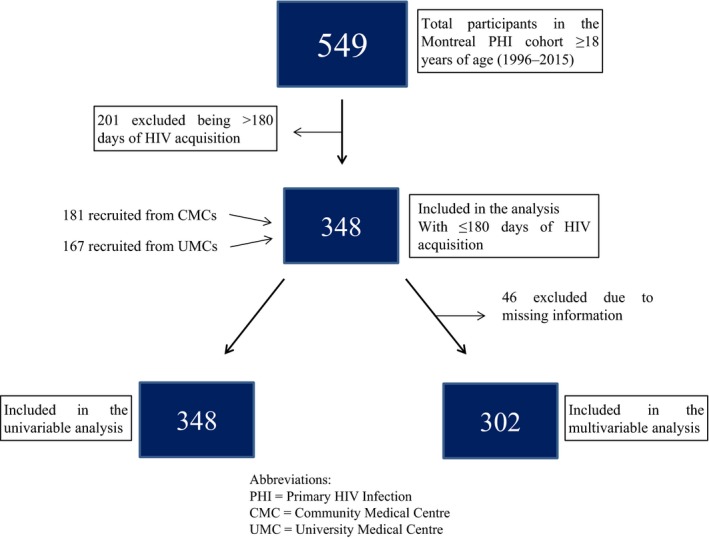
Methods: The Montreal Primary HIV Infection Study is a prospective cohort established in three community medical centres (CMCs) and two university medical centres (UMCs). Recently diagnosed HIV-infected adults were categorized as receiving early (vs. delayed) ART if ART was initiated within 180 days of the baseline visit. Associations between early ART initiation and socio-demographic, socio-economic and behavioural information were examined. Independent associations of factors linked with early ART initiation were determined using multivariable binary logistic regression analysis.
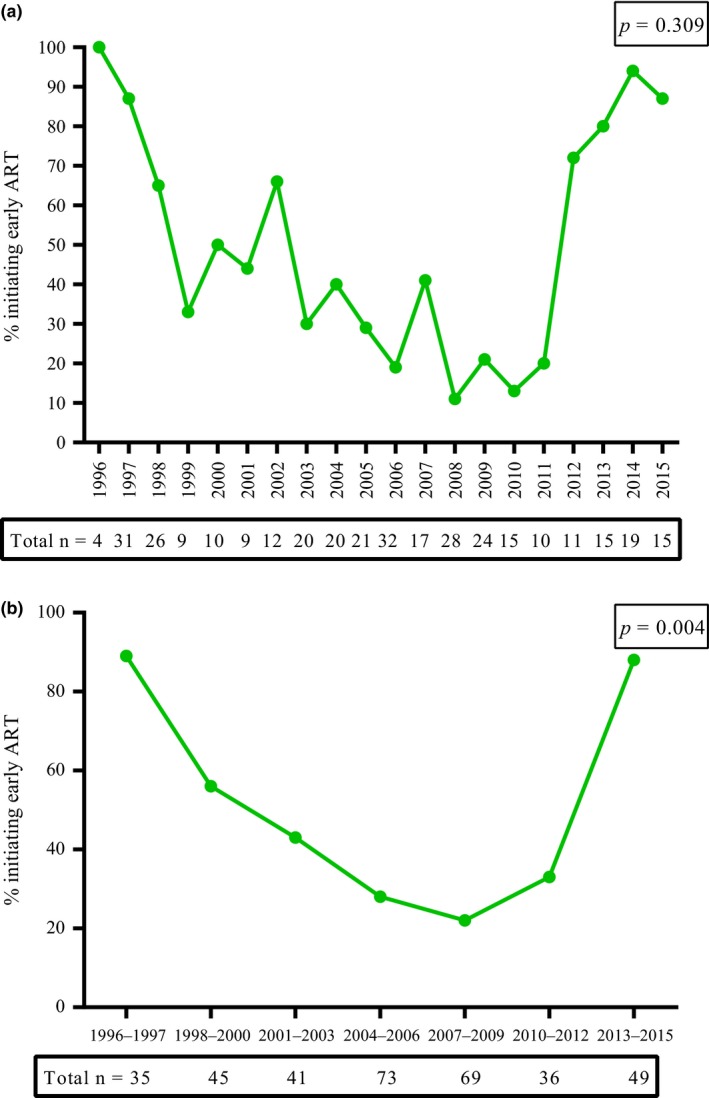
Results: A total of 348 participants had a documented date of HIV acquisition of <180 days. The median interquartile range (IQR) age of participants was 35 (28; 42) years and the majority were male (96%), having paid employment (63%), men who have sex with men (MSM) (78%) and one to four sexual partners in the last three months (70%). Participants presented with a median IQR HIV plasma viral load of 4.6 (3.7; 5.3) log10 copies/ml, CD4 count of 510 (387; 660) cells/μl and were recruited in CMCs (52%) or UMCs (48%). Early ART initiation was observed in 47% of the participants and the trend followed a V-shaped curve with peaks in 1996 to 1997 (89%) and 2013 to 2015 (88%) with a dip in 2007 to 2009 (22%). Multivariable analyses showed that having a paid employment adjusted odds ratio (aOR: 2.43; 95% CI: 1.19, 4.95), lower CD4 count (aOR per 50 cell increase: 0.93; 95% CI: 0.87, 0.99) and care at UMCs (aOR: 2.03; 95% CI: 1.06 to 3.90) were independently associated with early ART initiation.
Conclusions: Early ART initiation during primary HIV infection was associated with diminished biological prognostic factors and calendar time mirroring evolution of treatment guidelines. In addition, socio-economic factors such as having a paid employment, contribute to early ART initiation in the context of universal access to care in Canada.
Keywords: CD4 count; guidelines for the use of antiretroviral therapy; primary HIV infection; socio-demographic factors; socio-economic factors; time trends; universal access to care.
© 2018 The Authors. Journal of the International AIDS Society published by John Wiley & sons Ltd on behalf of the International AIDS Society.
Figures
References
-
- World Health Organization . Progress report 2016: prevent HIV, test and treat all, WHO support for country impact [cited 2017 Sep 29]. Available from: http://apps.who.int/iris/handle/10665/251713. 2016
-
- Montlahuc C, Guiguet M, Abgrall S, Daneluzzi V, de Salvador F, Launay O, et al. Impact of late presentation on the risk of death among HIV‐infected people in France (2003‐2009). J Acquir Immune Defic Syndr. 2013;64(2):197–203. - PubMed
-
- Sabin CA, Smith CJ, Gumley H, Murphy G, Lampe FC, Phillips AN, et al. Late presenters in the era of highly active antiretroviral therapy: uptake of and responses to antiretroviral therapy. AIDS. 2004;18(16):2145–51. - PubMed
-
- Brenner BG, Roger M, Routy JP, Moisi D, Ntemgwa M, Matte C, et al. High rates of forward transmission events after acute/early HIV‐1 infection. J Infect Dis. 2007;195(7):951–9. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
