

Immunogenic chemotherapy: Dose and schedule dependence and combination with immunotherapy
- PMID: 29414305
- PMCID: PMC5818299
- DOI: 10.1016/j.canlet.2018.01.050
Immunogenic chemotherapy: Dose and schedule dependence and combination with immunotherapy
Abstract
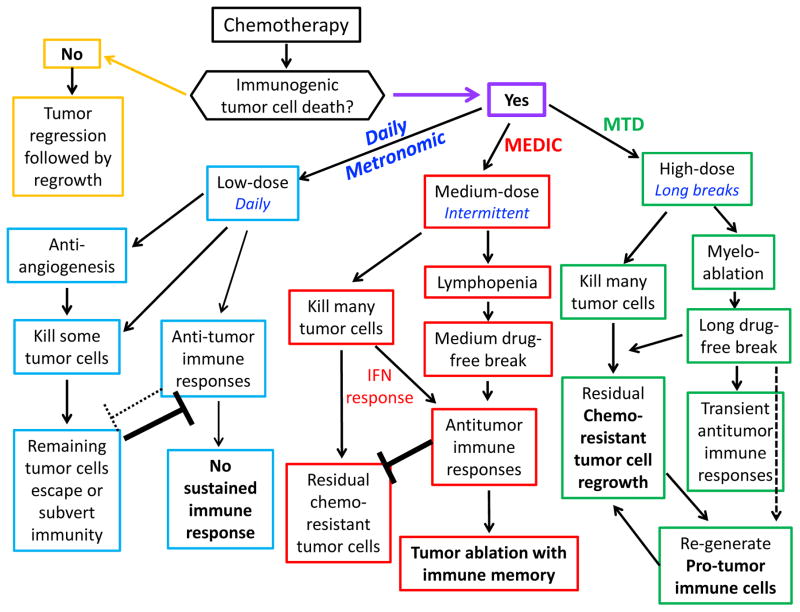
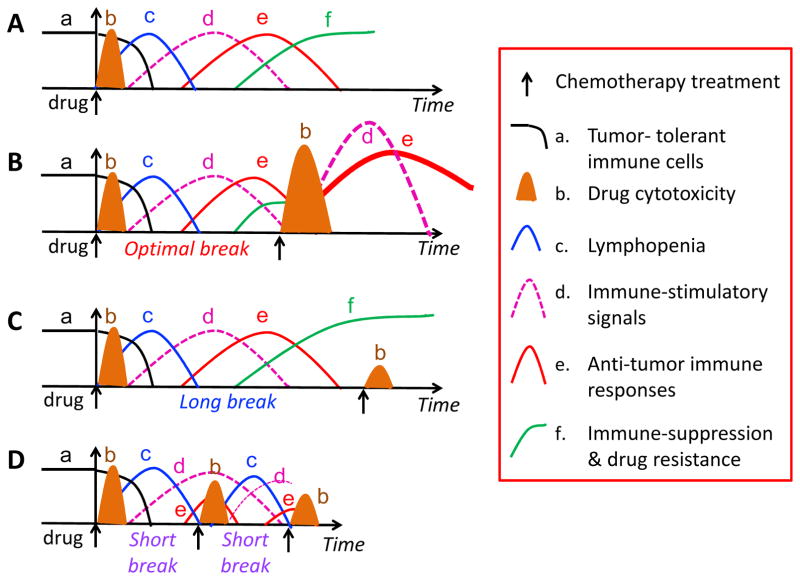
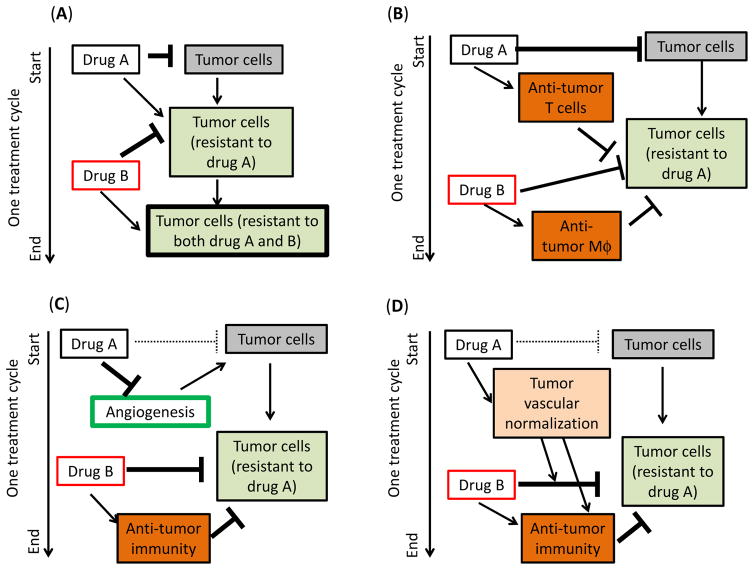
Conventional cytotoxic cancer chemotherapy is often immunosuppressive and associated with drug resistance and tumor regrowth after a short period of tumor shrinkage or growth stasis. However, certain cytotoxic cancer chemotherapeutic drugs, including doxorubicin, mitoxantrone, and cyclophosphamide, can kill tumor cells by an immunogenic cell death pathway, which activates robust innate and adaptive anti-tumor immune responses and has the potential to greatly increase the efficacy of chemotherapy. Here, we review studies on chemotherapeutic drug-induced immunogenic cell death, focusing on how the choice of a conventional cytotoxic agent and its dose and schedule impact anti-tumor immune responses. We propose a strategy for effective immunogenic chemotherapy that employs a modified metronomic schedule for drug delivery, which we term medium-dose intermittent chemotherapy (MEDIC). Striking responses have been seen in preclinical cancer models using MEDIC, where an immunogenic cancer chemotherapeutic agent is administered intermittently and at an intermediate dose, designed to impart strong and repeated cytotoxic damage to tumors, and on a schedule compatible with activation of a sustained anti-tumor immune response, thereby maximizing anti-cancer activity. We also discuss strategies for combination chemo-immunotherapy, and we outline approaches to identify new immunogenic chemotherapeutic agents for drug development.
Keywords: Anti-cancer drug scheduling; Anti-tumor immunity; Drug development; Immune memory; Immune suppression.
Copyright © 2018 Elsevier B.V. All rights reserved.
Conflict of interest statement
Figures
References
-
- Hanahan D, Coussens LM. Accessories to the crime: functions of cells recruited to the tumor microenvironment. Cancer Cell. 2012;21:309–322. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
