

An objective score to identify psychogenic seizures based on age of onset and history
- PMID: 29414562
- PMCID: PMC5845850
- DOI: 10.1016/j.yebeh.2017.11.035
An objective score to identify psychogenic seizures based on age of onset and history
Abstract
Objective: Psychogenic nonepileptic seizure (PNES) is a common diagnosis after evaluation of medication resistant or atypical seizures with video-electroencephalographic monitoring (VEM), but usually follows a long delay after the development of seizures, during which patients are treated for epilepsy. Therefore, more readily available diagnostic tools are needed for earlier identification of patients at risk for PNES. A tool based on patient-reported psychosocial history would be especially beneficial because it could be implemented in the outpatient clinic.
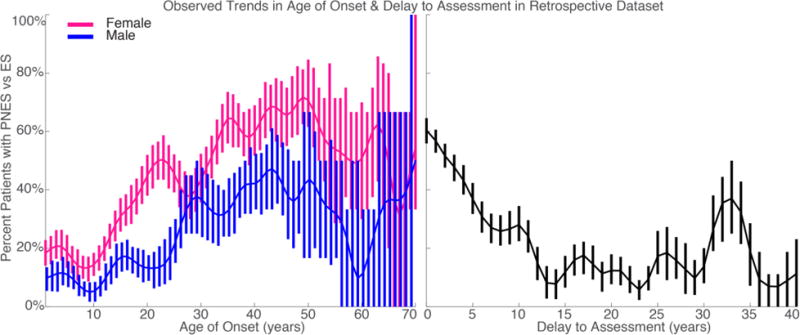
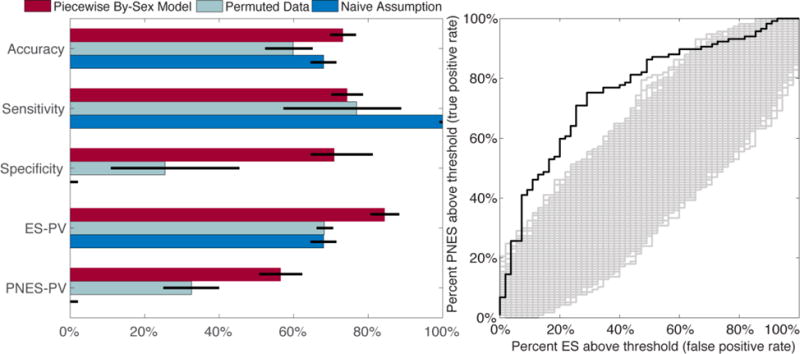
Methods: Based on the data from 1375 patients with VEM-confirmed diagnoses, we used logistic regression to compare the frequency of specific patient-reported historical events, demographic information, age of onset, and delay from first seizure until VEM in five mutually exclusive groups of patients: epileptic seizures (ES), PNES, physiologic nonepileptic seizure-like events (PSLE), mixed PNES plus ES, and inconclusive monitoring. To determine the diagnostic utility of this information to differentiate PNES only from ES only, we used multivariate piecewise-linear logistic regression trained using retrospective data from chart review and validated based on data from 246 prospective standardized interviews.
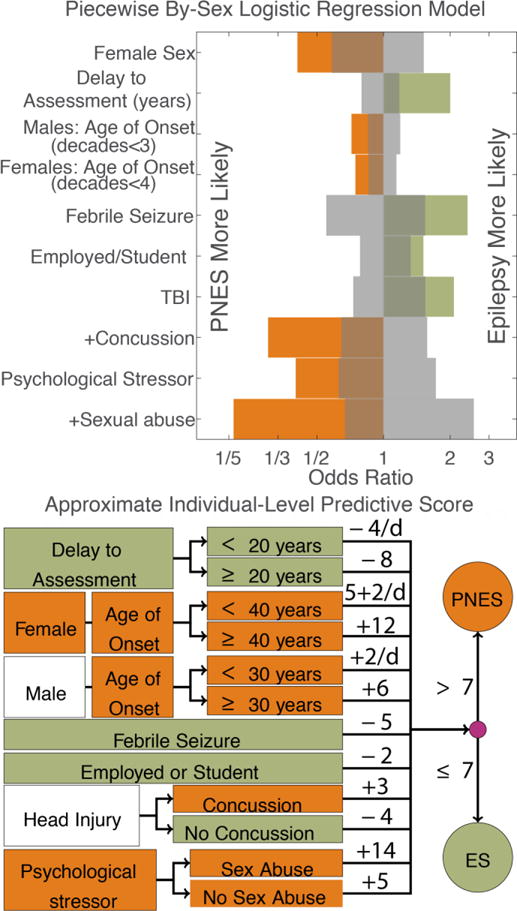
Results: The prospective area under the curve of our weighted multivariate piecewise-linear by-sex score was 73%, with the threshold that maximized overall retrospective accuracy resulting in a prospective sensitivity of 74% (95% CI: 70-79%) and prospective specificity of 71% (95% CI: 64-82%). The linear model and piecewise linear without an interaction term for sex had very similar performance statistics. In the multivariate piecewise-linear sex-split predictive model, the significant factors positively associated with ES were history of febrile seizures, current employment or active student status, history of traumatic brain injury (TBI), and longer delay from first seizure until VEM. The significant factors associated with PNES were female sex, older age of onset, mild TBI, and significant stressful events with sexual abuse, in particular, increasing the likelihood of PNES. Delays longer than 20years, age of onset after 31years for men, and age of onset after 40years for women had no additional effect on the likelihood of PNES.
Discussion: Our promising results suggest that an objective score has the potential to serve as an early outpatient screening tool to identify patients with greater likelihood of PNES when considered in combination with other factors. In addition, our analysis suggests that sexual abuse, more than other psychological stressors including physical abuse, is more associated with PNES. There was a trend of increasing frequency of PNES for women during childbearing years and plateauing outside those years that was not observed in men.
Keywords: Diagnostic score; Dissociative seizures; Logistic regression; Multiple imputation.
Copyright © 2017 Elsevier Inc. All rights reserved.
Conflict of interest statement
Conflicts & Ethical Publication:
Drs. Engel, Stern and Kerr have clinical responsibilities that include the diagnosis and treatment of patients with epilepsy and non-epileptic seizures. The remaining authors have no declared conflicts of interest. We confirm that we have read the Journal’s position on issues involved in ethical publication and affirm that this report is consistent with those guidelines.
Figures
References
-
- Dickinson P, Looper KJ. Psychogenic nonepileptic seizures: a current overview. Epilepsia. 2012;53:1679–89. - PubMed
-
- Alessi R, Valente KD. Psychogenic nonepileptic seizures: should we use response to AEDS as a red flag for the diagnosis? Seizure. 2014;23:906–8. - PubMed
-
- Razvi S, Mulhern S, Duncan R. Newly diagnosed psychogenic nonepileptic seizures: health care demand prior to and following diagnosis at a first seizure clinic. Epilepsy Behav. 2012;23:7–9. - PubMed
-
- Walczak TS, Papacostas S, Williams DT, Scheuer ML, Lebowitz N, Notarfrancesco A. Outcome after diagnosis of psychogenic nonepileptic seizures. Epilepsia. 1995;36:1131–7. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
