

Plasma Tryptophan-Kynurenine Metabolites Are Altered in Human Immunodeficiency Virus Infection and Associated With Progression of Carotid Artery Atherosclerosis
- PMID: 29415228
- PMCID: PMC6031054
- DOI: 10.1093/cid/ciy053
Plasma Tryptophan-Kynurenine Metabolites Are Altered in Human Immunodeficiency Virus Infection and Associated With Progression of Carotid Artery Atherosclerosis
Abstract
Background: It is unknown whether disrupted tryptophan catabolism is associated with cardiovascular disease (CVD) in human immunodeficiency virus (HIV)-infected individuals.
Methods: Plasma tryptophan and kynurenic acid were measured in 737 women and men (520 HIV+, 217 HIV-) from the Women's Interagency HIV Study and the Multicenter AIDS Cohort Study. Repeated B-mode carotid artery ultrasound imaging was obtained from 2004 through 2013. We examined associations of baseline tryptophan, kynurenic acid, and kynurenic acid-to-tryptophan (KYNA/TRP) ratio, with risk of carotid plaque.
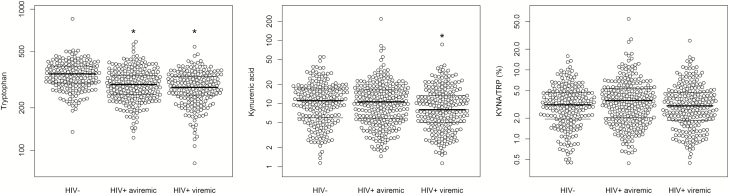
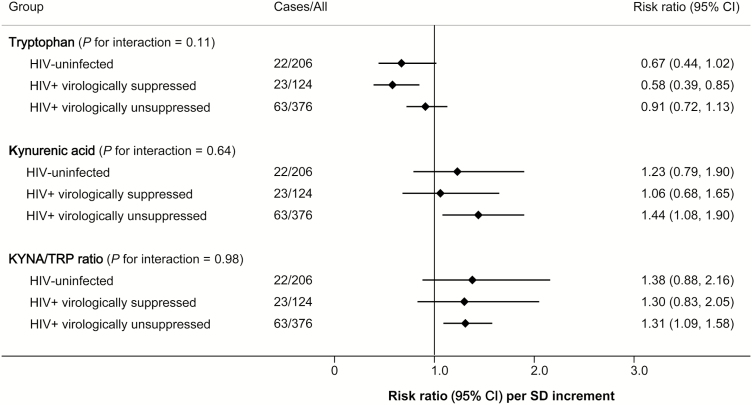
Results: After a 7-year follow-up, 112 participants developed carotid plaque. Compared to those without HIV infection, HIV-infected participants had lower tryptophan (P < .001), higher KYNA/TRP (P = .01), and similar kynurenic acid levels (P = .51). Tryptophan, kynurenic acid, and KYNA/TRP were correlated with T-cell activation (CD38+HLA-DR+) and immune activation markers (serum sCD14, galectin-3) but had few correlations with interleukin-6, C-reactive protein, or CVD risk factors (blood pressure, lipids). Adjusted for demographic and behavioral factors, each standard deviation (SD) increment in tryptophan was associated with a 29% (95% confidence interval [CI], 17%-38%) decreased risk of carotid plaque (P < .001), while each SD increment in kynurenic acid (P = .02) and KYNA/TRP (P < .001) was associated with a 34% (6%-69%) and a 47% (26%-73%) increased risk of carotid plaque, respectively. After further adjustment for CVD risk factors and immune activation markers, these associations were attenuated but remained significant.
Conclusions: Plasma tryptophan-kynurenine metabolites are altered in HIV infection and associated with progression of carotid artery atherosclerosis.
Figures
References
-
- Thienemann F, Sliwa K, Rockstroh JK. HIV and the heart: the impact of antiretroviral therapy: a global perspective. Eur Heart J 2013; 34:3538–46. - PubMed
-
- Huengsberg M, Winer JB, Gompels M, Round R, Ross J, Shahmanesh M. Serum kynurenine-to-tryptophan ratio increases with progressive disease in HIV-infected patients. Clin Chem 1998; 44:858–62. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- U01 AI035042/AI/NIAID NIH HHS/United States
- UL1 TR000424/TR/NCATS NIH HHS/United States
- P30 DK040561/DK/NIDDK NIH HHS/United States
- R01 HL132794/HL/NHLBI NIH HHS/United States
- U01 HD032632/HD/NICHD NIH HHS/United States
- R01 HL126543/HL/NHLBI NIH HHS/United States
- R01 HL095129/HL/NHLBI NIH HHS/United States
- U01 AI031834/AI/NIAID NIH HHS/United States
- U01 AI103397/AI/NIAID NIH HHS/United States
- U01 AI034994/AI/NIAID NIH HHS/United States
- UL1 TR000004/TR/NCATS NIH HHS/United States
- U01 AI035004/AI/NIAID NIH HHS/United States
- K01 HL137557/HL/NHLBI NIH HHS/United States
- U01 AI103390/AI/NIAID NIH HHS/United States
- P30 AI050410/AI/NIAID NIH HHS/United States
- R01 HL095140/HL/NHLBI NIH HHS/United States
- U01 AI103401/AI/NIAID NIH HHS/United States
- R01 HL083760/HL/NHLBI NIH HHS/United States
- U01 AI103408/AI/NIAID NIH HHS/United States
- K01 HL129892/HL/NHLBI NIH HHS/United States
- U01 AI034989/AI/NIAID NIH HHS/United States
- U01 AI034993/AI/NIAID NIH HHS/United States
- UL1 TR000454/TR/NCATS NIH HHS/United States
- R01 HL140976/HL/NHLBI NIH HHS/United States
- UL1 TR002378/TR/NCATS NIH HHS/United States
- U01 AI042590/AI/NIAID NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
