

Xanthine oxidase inhibitors for prevention of cardiovascular events: a systematic review and meta-analysis of randomized controlled trials
- PMID: 29415653
- PMCID: PMC5804046
- DOI: 10.1186/s12872-018-0757-9
Xanthine oxidase inhibitors for prevention of cardiovascular events: a systematic review and meta-analysis of randomized controlled trials
Abstract
Background: Xanthine oxidase inhibitors (XOI), classified as purine-like (allopurinol and oxypurinol) and non-purine (febuxostat and topiroxostat) XOI, present antioxidant properties by reducing the production of reactive oxygen species derived from purine metabolism. Oxidative stress is an important factor related to endothelial dysfunction and ischemia-reperfusion injury, and may be implicated in the pathogenesis of heart failure, hypertension, and ischemic heart disease. However, there is contradictory evidence regarding the possible cardiovascular (CV) protective effect exerted by XOI. Our objective is to compare the incidence of major adverse cardiovascular events (MACE), mortality, total (TCE) and specific CV events in randomized controlled trials (RCTs) testing XOI against placebo or no treatment.
Methods: PubMed, EMBASE, Web of Science, Cochrane Central, Lilacs databases were searched from inception to Dec 30 2016, along with hand searching. RCTs including exclusively adult individuals, lasting ≥ 4 weeks, with no language restriction, were eligible. Independent paired researchers selected studies and extracted data. Considering the expected rarity of events, Peto and DerSimonian/Laird odds ratios (OR), the latter in case of heterogeneity, were used for analysis. Random-effects meta-regression was used to explore heterogeneity.
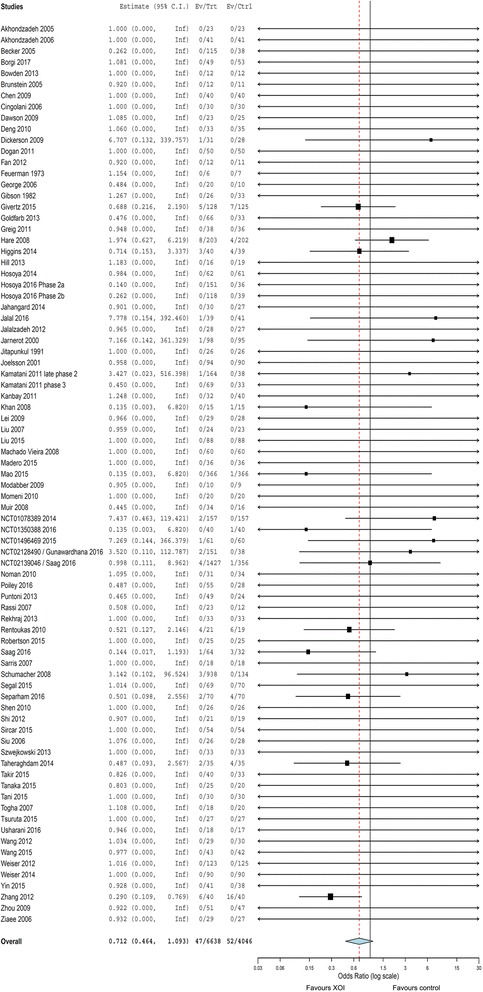
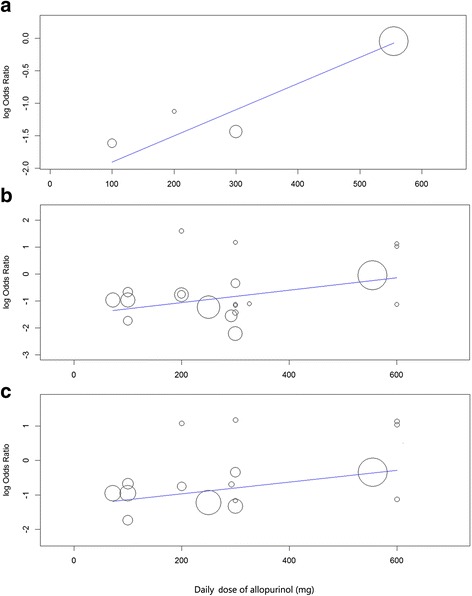
Results: The analysis of MACE included 81 articles (10,684 patients, 6434 patient-years). XOI did not significantly reduce risk of MACE (ORP = 0.71, 95% CI 0.46-1.09) and death (0.89, 0.59-1.33), but reduced risk of TCE (0.60, 0.44-0.82; serious TCE: 0.64, 0.46 to 0.89), and hypertension (0.54, 0.37 to 0.80). There was protection for MACE in patients with previous ischemic events (0.42, 0.23-0.76). Allopurinol protected for myocardial infarction (0.38, 0.17-0.83), hypertension (0.32, 0.18-0.58), TCE (0.48, 0.31 to 0.75, I2 = 55%) and serious TCE (0.56, 0.36 to 0.86, I2 = 44%). Meta-regression associated increasing dose of allopurinol with higher risk of TCE and serious TCE (P < 0.05). Accordingly, lower doses (≤ 300 mg/day) of allopurinol reduced the risk of TCE, unlike higher doses. Non-purine-like XOI did not significantly reduce or increase the risk of adverse CV events, but confidence intervals were wide. Quality of evidence was generally low to moderate.
Conclusions: Purine-like XOI may reduce the incidence of adverse CV outcomes. However, higher doses of allopurinol (> 300 mg/day) may be associated with loss of CV protection.
Keywords: Cardiovascular disease; Gout; Meta-analysis; Treatment; Xanthine Oxidase inhibitors.
Conflict of interest statement
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- MacIsaac RL, Salatzki J, Higgins P, Walters MR, Padmanabhan S, Dominiczak AF, et al. Allopurinol and cardiovascular outcomes in adults with hypertension. Hypertension. 2016;67:535–540. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
