

Characterizing undiagnosed chronic obstructive pulmonary disease: a systematic review and meta-analysis
- PMID: 29415723
- PMCID: PMC5803996
- DOI: 10.1186/s12931-018-0731-1
Characterizing undiagnosed chronic obstructive pulmonary disease: a systematic review and meta-analysis
Abstract
Background: A significant proportion of patients with chronic obstructive pulmonary disease (COPD) remain undiagnosed. Characterizing these patients can increase our understanding of the 'hidden' burden of COPD and the effectiveness of case detection interventions.
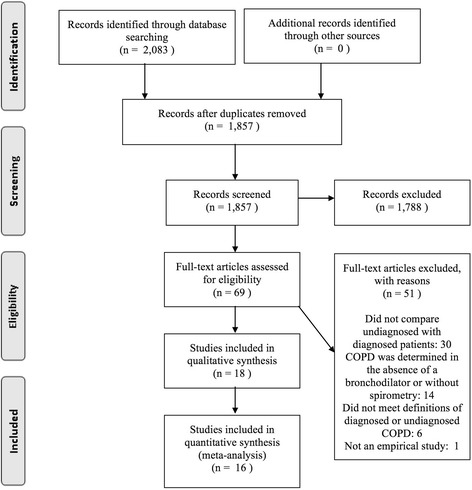
Methods: We conducted a systematic review and meta-analysis to compare patient and disease factors between patients with undiagnosed persistent airflow limitation and those with diagnosed COPD. We searched MEDLINE and EMBASE for observational studies of adult patients meeting accepted spirometric definitions of COPD. We extracted and pooled summary data on the proportion or mean of each risk factor among diagnosed and undiagnosed patients (unadjusted analysis), and coefficients for the adjusted association between risk factors and diagnosis status (adjusted analysis).
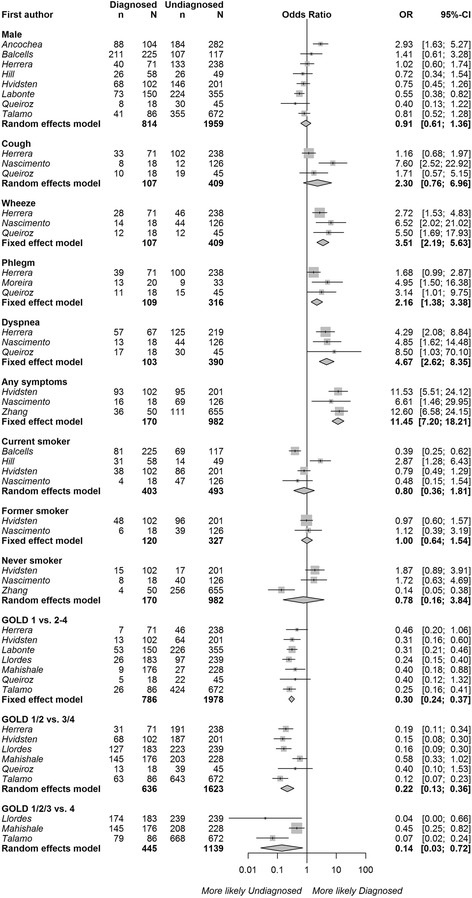
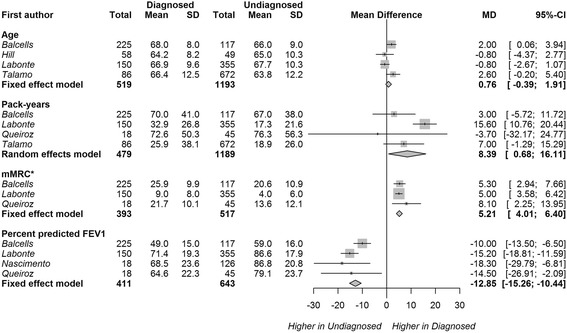
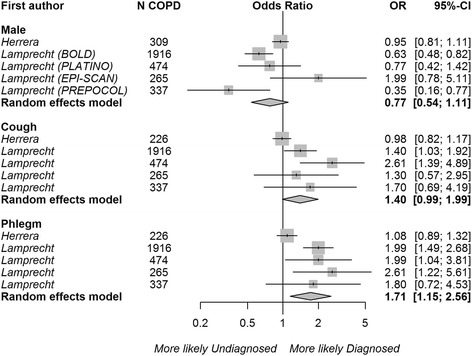
Results: Two thousand eighty-three records were identified through database searching and 16 articles were used in the meta-analyses. Diagnosed patients were less likely to have mild (v. moderate to very severe) COPD (odds ratio [OR] 0.30, 95%CI 0.24-0.37, 6 studies) in unadjusted analysis. This association remained significant but its strength was attenuated in the adjusted analysis (OR 0.72, 95%CI 0.58-0.89, 2 studies). Diagnosed patients were more likely to report respiratory symptoms such as wheezing (OR 3.51, 95%CI 2.19-5.63, 3 studies) and phlegm (OR 2.16, 95% CI 1.38-3.38, 3 studies), had more severe dyspnea (mean difference in modified Medical Research Council scale 0.52, 95%CI 0.40-0.64, 3 studies), and slightly greater smoking history than undiagnosed patients. Patient age, sex, current smoking status, and the presence of coughing were not associated with a previous diagnosis.
Conclusions: Undiagnosed patients had less severe airflow obstruction and fewer respiratory symptoms than diagnosed patients. The lower disease burden in undiagnosed patients may significantly delay the diagnosis of COPD.
Keywords: Chronic Obstructive Pulmonary Disease; Delayed diagnosis; Diagnostic errors; Differential diagnosis; Meta-analysis; Risk factors; Systematic review.
Conflict of interest statement
Ethics approval and consent to participate
Is not required because this study does not include analysis of individual data.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures

References
-
- From the Global Strategy for the Diagnosis, Management and Prevention of COPD . Global Initiative for Chronic Obstructive Lung Disease (GOLD) 2017.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
